Disasters and their Effects on the Population: Key Concepts
| Site: | Pediatric Pandemic Network Learn |
| Course: | Disasters and their Effects on the Population: Key Concepts |
| Book: | Disasters and their Effects on the Population: Key Concepts |
| Printed by: | Guest user |
| Date: | Wednesday, July 29, 2026, 4:18 PM |
1. Overview
Welcome to this multimedia open access edition of this chapter book titled Disasters and their Effects on the Population: Key Concepts.
This content is available as a digital book in two formats:
1) Website, which you are currently reading. This format offers a mobile friendly multimedia experience with sharable links to chapters. There are three ways to move through the book:
a) Use the table of contents chapter navigation to the left to navigate to different chapters in the book. Scroll through the links to select the chapter that interests you.
b) Use the yellow arrows that appear when scrolling to select previous and next chapters.
c) Use the previous chapter and next chapter buttons at the bottom of very page to navigate through the book.
2) Printable, which you can save as a PDF and open without an Internet connection.
1.1. Acknowledgements
Created by the Center for Global Health, Colorado School of Public Health
This content is owned by the Center for Global Health, Colorado School of Public Health, and has been jointly created by the Center for Global Health, Colorado School of Public Health and the Maternal and Child Health Department of Maimonides University; both of which are WHO Collaborating Centers in Maternal and Child Health. The course materials were developed with input from the American Academy of Pediatrics (AAP), the Pan American Health Organization (PAHO), and the Association for Health Research & Development (ACINDES).
With Support from the Pediatric Pandemic Network

The Pediatric Pandemic Network is supported in part by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) as part of cooperative agreements U1IMC43532 and U1IMC45814 with 0 percent financed with nongovernmental sources. The content presented here is that of the authors and does not necessarily represent the official views of, nor an endorsement by HRSA, HHS, or the U.S. Government. For more information, visit HRSA.gov.
Attribution-NonCommercial-NoDerivatives CC BY-NC-ND
You are free to download and share this work for noncommercial purposes, as long as you credit the Center for Global Health and the Pediatric Pandemic Network for the original creation.
2. Introduction
Book Authors
Patrick Mahar, MD | Col. Julia A. Lynch, MD, FAAP | Joseph Wathen, MD | Eric Tham, MD, MS, FAAP | Stephen Berman, MD, FAAP | Sathyanarayanan Doraiswamy, MD | Allen G.K. Maina, MD
Introduction
Recent advances in technology and the ease with which news and information travel around the world have made learning about disasters in distant countries an almost weekly occurrence. From the recent conflicts in Syria, Iraq, South Sudan, and the Central African Republic to the typhoon in the Philippines and flooding in the Zambezi region, these disasters have led to unimaginable levels of destruction and death.
Although most of these disasters occur in underserved areas of the world without adequate resources and technology, they can also occur in societies with advanced medical systems such as the United States, Europe, and Japan. It is impossible to predict when and where the next disaster will take place. However, we can strive to be prepared to handle both the acute and longer-term effects of a variety of disasters in different populations.
While the timing and the actual disaster event are difficult to predict, several consequences of disasters are predictable. Therefore, we can prepare to deal with these consequences. As pediatricians, we must ensure that disaster preparedness includes the unique needs of children. Children are a vulnerable population with physiologic, psychological, and developmental needs that differ from those of adults.
There is a professional obligation to take an active role in disaster preparedness in order to advocate for the needs of infants, children, and teenagers.
Learning Objectives
In this module, we will:
- Review disaster definitions, classifications, and measures of severity
- Describe the phases of a disaster
- Review World Health Organization recommended emergency response measures
- Discuss the role of humanitarian organizations
- Present key issues that health care workers and medical volunteers may face in disaster relief
Key Takeaway
The key message of this module is that while it is not possible to predict disasters, planning and preparation can help mitigate some of the morbidity and mortality that occur in the aftermath of a disaster.
“Failing to plan is planning to fail.” — Benjamin Franklin
3. Definitions
Objectives
- Recognize events that can lead to disasters.
- Understand the individual and social factors associated with vulnerability, coping, and risk.
Case
You are informed there has been a flood affecting one of the areas of your country. According to the latest population census, around 200,000 people who are mostly poor live in this area.
Twenty-five percent of the population affected by the flood are children aged 0–12 years old. This population is more vulnerable than others in disaster situations.
After arriving at the flooded area, you must decide what to do to deliver health care to the victims.
Reflection Questions
- What characteristics indicate that this event can be defined as a disaster?
- What type of disaster is it?
- What characteristics make children more vulnerable?
- What specific interventions are necessary to diminish the effects of disaster upon children?
- What is the first step to be taken?
- How useful are field hospitals in these situations?
- How would you estimate the need for external help?
What Makes an Event a Disaster?
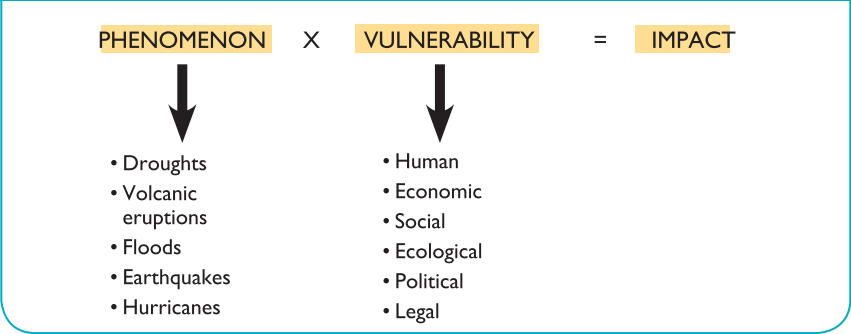
What makes an event a disaster? Why is one hurricane or tornado a disaster and the next one, even with stronger winds, is just a bad storm? The answer lies with how the population is eventually affected: both the direct effects on the people as well as the indirect effects or damage to infrastructure. The United Nations International Strategy for Disaster Reduction defines disaster as a serious disruption of the functioning of a community or a society involving widespread human, material, economic or environmental losses and impacts, which exceeds the ability of the affected community or society to cope using its own resources.
Key Concept: Any adverse episode or phenomenon can exploit a vulnerability in the affected population or community to create damage, and this awareness will form the basis for an adequate intervention.
Disasters are often described as a result of the combination of: exposure to a hazard; the conditions of vulnerability that are present; and insufficient capacity or measures to reduce or cope with the potential negative consequences. Disaster impacts may include loss of life, injury, disease and other negative effects on human physical, mental and social well-being, together with damage to property, destruction of assets, loss of services, social and economic disruption and environmental degradation.
A disaster disrupts the normal pattern of life, causing both physical and emotional suffering and an overwhelming sense of helplessness and hopelessness. The impact on the socioeconomic structure of a region and environment often requires outside assistance and intervention. Although there are many definitions for disaster, there are three common factors.
Box 1. Definitions of a Disaster
“A disaster is a crisis resulting from a failure in human interactions with the physical and social environment. Disaster situations outstrip the capacity of individuals and societies to cope with adversity”.
HDI, From Disaster Relief to Development, Studies on Development, No 1 (Geneva: Henry Dunant Institute, 1988), p. 170.
“A disaster is the convergence, at a given moment and in a given place, of two factors: risk and vulnerability”.
G. Wilches-Chaux, “La vulnerabilidad global,” in Herramientas para la crisis: Desastres, ecologismo y formación profesional (Popayan, Colombia: Servicio Nacional de Aprendizaje [SENA], Sept. 1989).
“A disaster has occurred when the destructive effects of natural or man-made forces overwhelm the ability of a given area or community to meet the demand for health care.”
Mothershead JL et al. Disaster Planning. Available at: http://www.emedicine.com/emerg/topic718.htm#section~definitions_and_terminology.
“A disaster can be defined as a serious disruption of the functioning of a society, causing widespread human, material or environmental losses which exceed the ability of the affected society to cope using only its own resources.”
Bryce, C.P. “Stress management in disasters”, Washington D.C, OPS, 2001.
Common Factors
First, there is an event or phenomenon that impacts a population or an environment. Second, a vulnerable condition or characteristic allows the event to have a more serious impact.
For example, a hurricane will cause much greater damage to life and structures if it directly strikes an area with poorly constructed dwellings compared to striking a community of well-built homes with greater structural support. Identifying these factors has practical implications for communities’ preparedness and provides a basis for prevention.
Third, local resources are often inadequate to cope with the problems created by the phenomenon or event. Disasters affect communities in multiple ways. Their impact on the health care infrastructure is also multifactorial. The disaster event can cause an unexpected number of deaths. In addition, the large numbers of wounded and sick often exceed the local community’s health care delivery capacity.
Health Care Infrastructure Impact
The community’s capacity to care for those affected is often reduced because professionals, clinics and hospitals have been affected or destroyed. This will have long-term consequences leading to increased morbidity and mortality. An example of this can be seen in the 2010 Haiti earthquake disaster.
Real-World Example: Haiti Earthquake
Prior to the January 12, 2010 earthquake in Haiti there were only 11 hospitals in Port-au-Prince. The earthquake damaged or destroyed at least eight of these hospitals. The remaining health facilities were quickly overwhelmed by large numbers of survivors requiring a wide range of care, particularly for traumatic injuries.
The Haiti earthquake demonstrates how a disaster becomes much more devastating when the preexisting medical system is already inadequate and poorly functional. This makes integrating and organizing outside assistance more fragmented and chaotic.
Real-World Example: Ebola Epidemic
An epidemic or pandemic can cause a surge in the number of people seeking medical care and thus overwhelm the abilities of even a well-established medical system. The Ebola epidemic in West Africa is an example of how a disaster can affect the rest of the world.
Environmental, Psychological, and Social Effects
Disasters can also have adverse effects on the environment that increase the risk for infectious diseases and environmental hazards. The loss of clean drinking water and proper sewage treatment can have devastating effects on affected populations. Food shortages can lead to severe nutritional consequences.
All these conditions may create a sense of hopelessness, vulnerability and an inability to envision a better future. People may stop planning their future such as finishing school, getting married or working. This “foreshortened future” affects the psychological and social behavior of the community. (Figure 1)
Adapted from Handbook of War and Public Health; ICRC; 1996.
3.1. Classification of disasters
Types of Disasters
Disasters can be divided into 2 large categories (Box 2):
- Those caused by natural forces.
- Those caused by man.
Box 2: Types of disasters
Natural disasters
- Hurricanes or cyclones
- Tornadoes
- Floods
- Avalanches and mud slides
- Tsunamis
- Hailstorms
- Droughts
- Forest fires
- Earthquakes
- Epidemics
Man-provoked disasters
Technological/industrial disasters
- Leaks of hazardous materials
- Accidental explosions
- Bridge or road collapses, or vehicle collisions
- Power cuts
Terrorism/International violence
- Bombs or explosions
- Release of chemical materials
- Release of biological agents
- Release of radioactive agents
- Multiple or massive shootings
- Mutinies
- Intentional fires
Complex emergencies
- Conflicts or wars
- Genocide
Modified from Lou Romig, Disaster Management, in APLS, 4TH Edition, J&B Publishers, 2004
Natural disasters
Natural disasters are caused by natural forces such as earthquakes, volcanic eruptions, hurricanes, fires, tornadoes, and extreme temperatures.
They can be classified as rapid-onset disasters, such as earthquakes or tsunamis, and those with progressive onset, such as droughts that may lead to famine.
These events, usually sudden, can have tremendous effects. For instance, in November 2013, more than 6,000 people died and over 4 million were displaced in the Philippines as a result of Typhoon Haiyan.
Usually, a great number of persons die when a complex humanitarian emergency occurs
Since it is still extremely difficult to precisely predict the climatic and geological changes capable of causing a disaster, preparing for these types of events remains a major challenge.
Great natural disasters have also occurred recently throughout the world. (Box 3).
BOX 3. Natural disasters in the Americas in 2013
Heat Waves
Bolivia (August 2013): 17,490 people affected; 18 deaths
Earthquakes
Colombia (September 2013): 3,957 people affected
Peru (September 2013): 7,084 people affected
Epidemics
Costa Rica (July 2013, viral outbreak): 1,200 people affected; 3 deaths
Guatemala (August 2013, viral outbreak): 1,977 people affected; 8 deaths
Floods
Argentina (July 2013): 350,000 people affected; 52 deaths
Bolivia (February 2013): 145,000 people affected; 25 deaths
Brazil (January 2013): 200,000 people affected; 4 deaths
Peru (February 2013): 180,766 people affected; 67 deaths
Volcanic Eruptions
El Salvador (December 2013): 63,079 people affected
Tornado
USA – Oklahoma City (May 2013): 370 injured; 26 deaths
Modified from EM-DAT The International Disaster Database
The inability to accurately predict these types of events underscores the need for countries to have disaster response plans to mobilize appropriate resources rapidly and efficiently. A well-defined organizational structure must also be created to coordinate both national and international assistance.
Although significant progress in sanitation and disaster response has been achieved in certain regions of the world, developing countries continue to be highly vulnerable because of their fragile economies and limited healthcare and transportation infrastructure.
Man-made disasters
Disasters caused by humans are those in which the major direct causes are identifiable as intentional or unintentional human actions. They can be subdivided into three main categories:
Technological disasters
Unregulated industrialization and inadequate safety standards increase the risk of industrial disasters. Examples include the radioactive leak at the Chernobyl nuclear power plant in Ukraine (1986) and the toxic gas leak at a factory in Bhopal, India (1984). Both of these disasters were associated not only with many deaths but also with long-term health effects in the affected population.
Terrorism/Violence
The threat of terrorism has increased due to the spread of technologies involving nuclear, biological, and chemical agents used to develop weapons of mass destruction. Too often, the professionals who must respond to such disasters are not adequately trained, although several national and international organizations are developing training programs for these types of events.
Complex humanitarian emergencies
The term complex emergency is usually used to describe the humanitarian emergency resulting from an international or civil war. In such situations, large numbers of people are displaced from their homes because of the lack of personal safety and the disruption of basic infrastructure, including food distribution, water, electricity, and sanitation. In other cases, communities are left stranded and isolated in their own homes, unable to access assistance.
These settings are often characterized by a breakdown in social and physical infrastructure, including healthcare systems. Any emergency response usually has to be implemented in a difficult political and security environment.
There has been a global increase in civil war fueled by ethnic confrontations since the mid-1990s (Figure 2). In modern conflicts, the greatest loss of life (90%) occurs among civilian non-combatants because of direct physical injury and the public health impact of war (Figure 3).
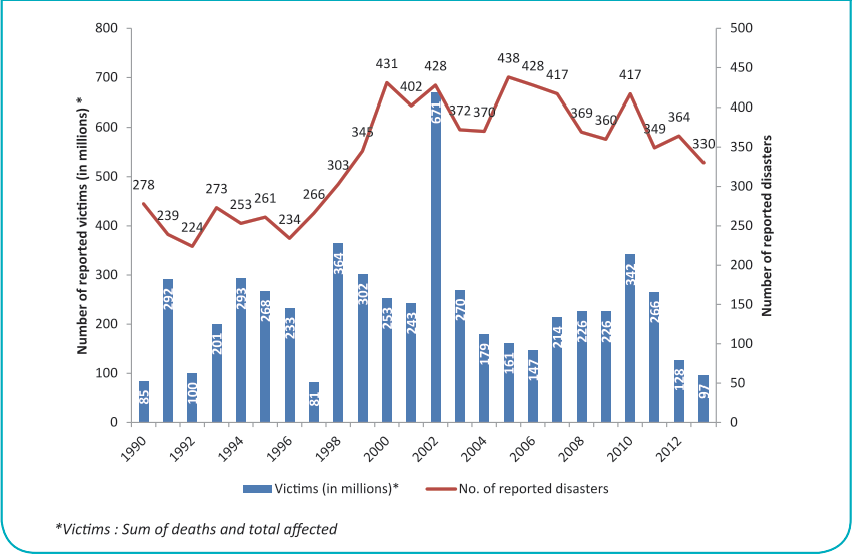
Source: “Annual Disaster Statistical Review 2013: The numbers and trends.” Debarati Guha-Sapir, Philippe Hoyois and Regina Below http://reliefweb.int/sites/reliefweb.int/files/resources/ADSR_2013.pdf
Source: “War’s Human Cost.” UNHCR Global Trends 2013. http://www.unhcr.org/5399a14f9.html
Complex humanitarian emergencies often result in a staggering loss of life. Table 1 shows the estimated excess deaths among civilians in several recent and ongoing crises.
| Country | Deaths | Period |
|---|---|---|
| Sudan | Over 1 million | 1983 to date |
| Rwanda | 500,000–1 million | 1994 to date |
| Cambodia | Over 1 million | 1975–1993 |
| Bosnia-Herzegovina | 200,000 | 1992–1996 |
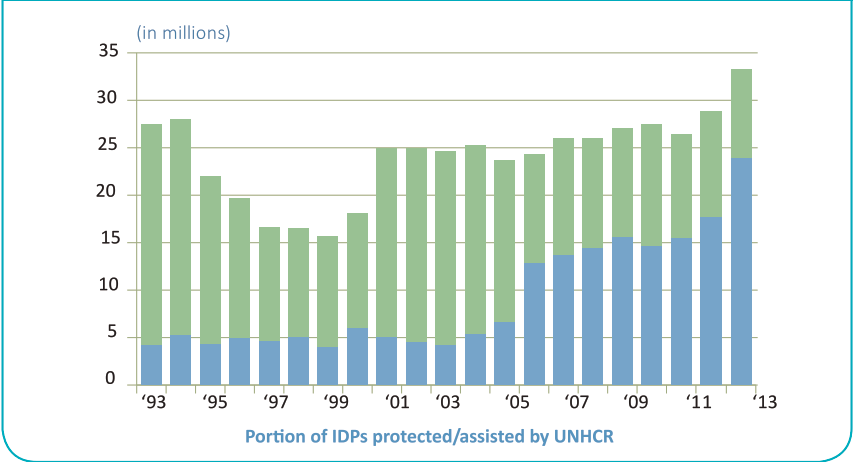
Displaced Populations
Natural disasters and complex emergencies can force many people to leave their homes. The primary purpose of the United Nations High Commissioner for Refugees (UNHCR) is to safeguard the rights and well-being of people who have been forced to flee, including the right to seek asylum and find safe refuge in another country. Refugees and internally displaced persons (IDPs) are among the categories of people that UNHCR assists.
Refugees flee their countries because of war, violence, famine, or a well-founded fear of persecution for political, ethnic, religious, or nationality-related reasons. According to 2015 UNHCR estimates, there are 21.3 million refugees and 10 million stateless people (Figure 5). A person recognized as a refugee is entitled to certain protections under the terms of international humanitarian law.
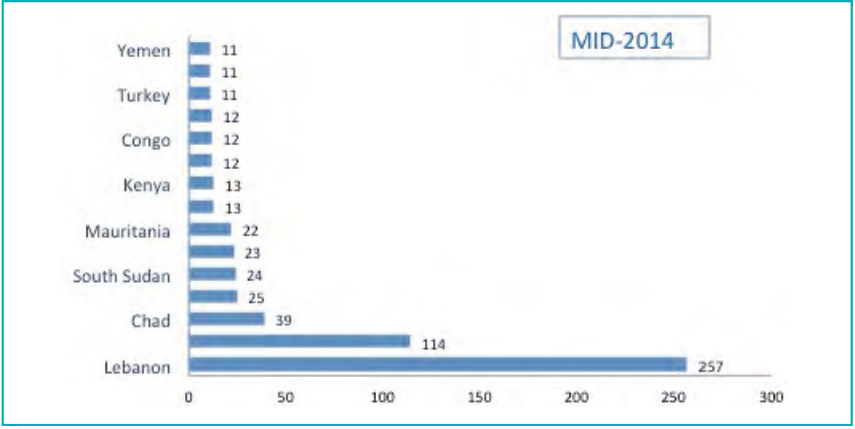
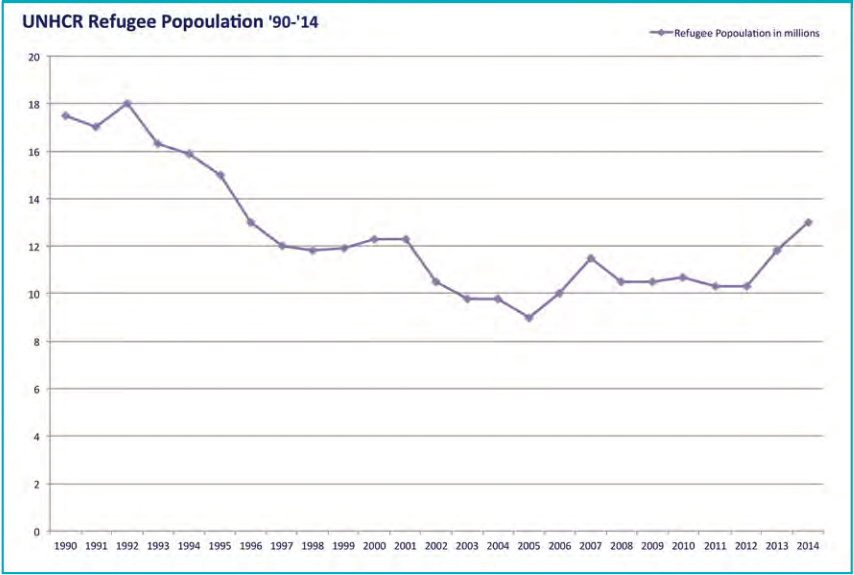
Internally displaced persons (IDPs) leave their homes for similar reasons but do not cross the boundaries of their countries. These individuals do not receive the same kind of legal protection, which can make assisting them more difficult. According to the 2015 Internal Displacement Monitoring Centre, there are 65.3 million displaced people.
More information is available at:
3.2. Phases of disasters
Phases of Disaster Intervention
Since interventions in emergencies evolve as a continuum, identifying the following four phases is useful for establishing priorities, guiding response activities, and systematizing previous experiences:
- Preparedness phase
- Response phase
- Recovery phase
- Mitigation and prevention phase
Preparedness phase
Planning comprises all activities and actions taken in advance of a disaster. It should be based on an analysis of a community’s or organization’s risk of exposure to specific types of disasters.
Preparedness plans should take into account the frequency of occurrence of each type of disaster, the anticipated magnitude of impact, the degree of advance warning or suddenness of onset and offset, the characteristics of populations most likely to be affected, the amount and types of resources available, and the ability to function independently without external support for a period of time.
For more information on planning, see Module 3.
Response phase
The response phase comprises all activities and actions taken during and immediately after a disaster. This includes notification of relevant organizations, establishment of communication networks, search and rescue operations, damage assessment, evacuation, sheltering, and other critical activities.
This phase lasts until initial casualties have been rescued or accounted for, and sufficient resources are available to meet the immediate humanitarian needs of the affected population. It also includes assessing damage and beginning to plan for restoration and recovery.
In conflict situations, displacement may be prolonged until safety and security are restored. Affected populations may need to be supported in camps designed for temporary accommodation. While normal conditions after natural disasters may return within days or weeks, in conflict settings it may take years before people can return to their homes.
Recovery phase
The recovery phase is the period during which the affected organization or community works toward re-establishing self-sufficiency. This includes community planning, rebuilding, and the re-establishment of government and public service infrastructure.
The health status of the affected population begins to return to pre-disaster conditions, and external support services are gradually withdrawn.
Mitigation and prevention phase
This phase usually occurs as conditions return to their pre-disaster state. Mitigation involves reviewing all aspects of emergency management to identify lessons learned and applying them to prevent recurrence or reduce the impact of future disasters.
Mitigation includes preventive and precautionary measures such as improving building codes and practices, redesigning public utilities and services, reviewing evacuation procedures and warning systems, and educating communities.
Mitigation and planning are continuous processes, as lessons learned from previous disasters are incorporated into future preparedness efforts.
3.3. Effects of disasters
Effects of Disasters
Disasters affect communities in multiple ways. They represent a public health hazard for various reasons (Table 2):
- They can cause an unexpected number of deaths and injured or sick people that exceed local response capacity and require external aid.
- They can destroy health infrastructure, affecting the immediate response and disrupting preventive activities, which may lead to long-term increases in morbidity and mortality.
- They can have adverse effects on the environment, increasing the risk of infectious diseases and environmental hazards. This can affect morbidity, premature death, and future quality of life.
- They can affect the psychological and social behavior of the community.
- They can cause shortages of food, with severe nutritional consequences.
- They can cause large population movements, whether spontaneous or organized, to areas where health services may be unable to meet increased demand.
Table 2. Frequent effects of disasters by type
Select each disaster type to review its frequent effects. For printing, expand all sections before printing.
Complex emergency
| Immediate deaths | Numerous |
|---|---|
| Severe lesions | Numerous |
| Increased risk for transmissible diseases | This risk applies to all significant disasters and increases with overcrowding and deterioration of sanitary conditions. |
| Damage to health centres | Moderate; can be severe if health centers are military targets |
| Damage to water supply | Severe |
| Food shortage | Severe |
| Significant population displacements | Frequent |
Earthquake
| Immediate deaths | Numerous |
|---|---|
| Severe lesions | Numerous |
| Increased risk for transmissible diseases | This risk applies to all significant disasters and increases with overcrowding and deterioration of sanitary conditions. |
| Damage to health centers | Severe |
| Damage to water supply | Severe |
| Food shortage | May result from economic and logistic factors |
| Significant population displacements | Frequent; increased likelihood in severely damaged urban areas |
Strong winds
| Immediate deaths | Few |
|---|---|
| Severe lesions | Moderate |
| Increased risk for transmissible diseases | This risk applies to all significant disasters and increases with overcrowding and deterioration of sanitary conditions. |
| Damage to health centers | Severe |
| Damage to water supply | Slight |
| Food shortage | May result from economic and logistic factors |
| Significant population displacements | Not frequent |
Floods
| Immediate deaths | Numerous |
|---|---|
| Severe lesions | Few |
| Increased risk for transmissible diseases | This risk applies to all significant disasters and increases with overcrowding and deterioration of sanitary conditions. |
| Damage to health centers | Severe but localized |
| Damage to water supply | Severe |
| Food shortage | Frequent |
| Significant population displacements | Frequent |
Gradual floods
| Immediate deaths | Few |
|---|---|
| Severe lesions | Few |
| Increased risk for transmissible diseases | This risk applies to all significant disasters and increases with overcrowding and deterioration of sanitary conditions. |
| Damage to health centers | Severe (equipment only) |
| Damage to water supply | Slight |
| Food shortage | Frequent |
| Significant population displacements | Frequent |
Mudslides
| Immediate deaths | Numerous |
|---|---|
| Severe lesions | Few |
| Increased risk for transmissible diseases | This risk applies to all significant disasters and increases with overcrowding and deterioration of sanitary conditions. |
| Damage to health centers | Severe but localized |
| Damage to water supply | Severe but localized |
| Food shortage | Not frequent |
| Significant population displacements | Frequent |
Volcanic Eruptions
| Immediate deaths | Numerous |
|---|---|
| Severe lesions | Few |
| Increased risk for transmissible diseases | This risk applies to all significant disasters and increases with overcrowding and deterioration of sanitary conditions. |
| Damage to health centers | Severe |
| Damage to water supply | Severe |
| Food shortage | Not frequent |
| Significant population displacements | Frequent |
Adapted from Humanitarian Assistance in Disaster Situations. A Guide for Effective Aid. Pan-American Health Organization (PAHO). Washington D.C., 1999.
4. Mortality
OBJECTIVES
- Recognize crude mortality and under 5 mortality rates as a measure of disaster severity.
- Recognize the environmental factors associated with increased morbidity and mortality rates.
- Know the 5 leading causes of death in humanitarian emergencies occurring in developing countries.
Severity of a disaster
As was demonstrated in Haiti, the more fragile the pre-event health status of the affected population and the more inadequate the pre-disaster infrastructure, the more severe the disaster. Disaster severity therefore varies according to its magnitude and the vulnerability of the population.
Most diseases associated with the event can be prevented by adequate interventions, especially ensuring basic life saving needs of the population are met. This includes shelter, food, water, sanitation, health care services and security measures.
An example of this can be seen in earthquakes of similar magnitude in different parts of the world. Earthquakes in China and Haiti resulted in a large number of collapsed buildings, including schools and hospitals, related to substandard building practices in both countries, and thus a high number of casualties. By contrast, earthquakes of similar magnitude occurring in Tokyo in 2009 and Chile in 2010 resulted in far less loss of life, largely because of higher-quality construction and stricter building codes.
Crude mortality rate
When assessing the outcome of a disaster, public health officers describe its severity by the number of human lives lost using the crude mortality rate (CMR). CMR is usually defined as the number of deaths per 10,000 inhabitants per day.
Natural disasters can result in numerous immediate deaths due to trauma
In developing countries, the reference CMR value varies from 0.4 to 0.7 deaths per 10,000 people per day. A CMR above 1 death per 10,000 people per day, or an under-5 mortality rate above 2 deaths per 10,000 children under 5 per day, is considered a humanitarian emergency.
While both conflicts and natural disasters can result in immediate deaths due to trauma or drowning, there are many preventable deaths that occur in later phases of a disaster over a longer time period.
To assess the progression of a disaster and the effectiveness of relief interventions, the CMR should be measured over several appropriate time intervals. For example, during the month following the massive movement of Rwandan refugees to eastern Zaire (present-day Democratic Republic of the Congo), the CMR in that region was 40 to 60 times above the corresponding reference value.
The CMR is usually highest during the initial phase of a disaster. Figure 6 displays the differences between baseline and peak disaster CMR experienced by displaced populations in different countries. Additional information regarding these epidemiologic measurements may be found in Module 2, “Preventive Medicine in Humanitarian Emergencies.”
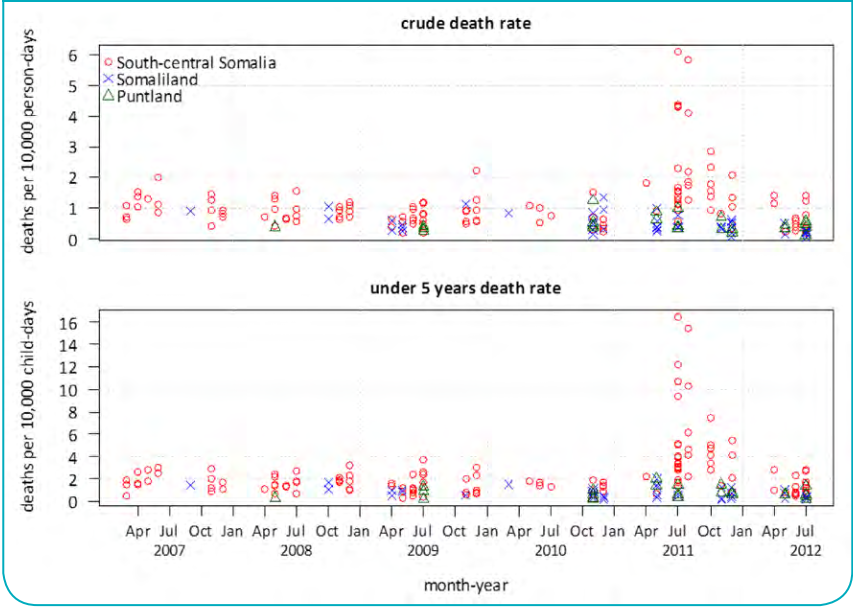
Source: “Mortality among populations of southern and central Somalia affected by severe food insecurity and famine during 2010–2012.” A study commissioned by FAO/FSNAU and FEWS NET, conducted by the London School of Hygiene and Tropical Medicine and the Johns Hopkins University Bloomberg School of Public Health.
4.1. Vulnerable victims
Vulnerable Populations During Disasters
Most diseases associated with disasters can be prevented by adequate interventions, especially by ensuring that the basic life-saving needs of the population are met. These include shelter, food, water, sanitation, healthcare services, and security measures.
Immediate mortality in any type of disaster is not higher in a specific age group; instead, it usually reflects the age distribution of the overall population. However, in later stages, mortality rates tend to be disproportionately higher among the youngest and oldest people. For example, during the refugee crisis in Northern Iraq in 1991, children aged 0 to 5 accounted for only 18% of the total refugee population but represented 64% of overall refugee mortality.
The most vulnerable groups include children, especially those separated from their families; pregnant or lactating women; women living without their spouses; individuals in female-headed households; people with disabilities; and the elderly.
In addition to disproportionately high mortality rates, children separated from their families are at high risk of adverse consequences such as violence, exploitation, and abuse, including child labor, trafficking, and recruitment as child soldiers. Furthermore, infants and children are more vulnerable to toxic exposures and overcrowding associated with large population displacements (Table 3).
Table 3. Vulnerable pediatric characteristics
| Pediatric characteristic | Special risk during disaster |
|---|---|
| Respiratory | Higher minute ventilation increases exposure to inhaled agents. Nuclear fallout and heavier gases settle closer to the ground and may affect children more severely. |
| Gastrointestinal | Higher risk of dehydration from vomiting and diarrhea after exposure to contaminated food or water. |
| Skin | Greater body surface area increases exposure risk. Skin is thinner and more susceptible to burns, chemicals, and toxin absorption. Increased evaporation also raises the risk of hypothermia. |
| Endocrine | Increased risk of thyroid cancer following radiation exposure. |
| Thermoregulation | Reduced ability to regulate body temperature, increasing the risk of hypothermia. |
| Developmental | Limited ability to recognize or escape environmental dangers. |
| Psychological | Higher vulnerability to prolonged stress and separation anxiety. |
Consequently, it is critical to reunite children with their families as soon as possible and to prioritize reducing their vulnerability in all disaster response planning (Box 4).
BOX 4. Immediate measures developed to reduce population vulnerability during a disaster
- List vulnerable individuals in the community.
- Provide visible identification tags for all children.
- Identify community leaders—preferably women—capable of caring for vulnerable individuals or groups.
- Ensure the care and safety of refugees.
- Consider vulnerable individuals when planning distribution systems.
- Prioritize locating families of unaccompanied or vulnerable individuals.
- Display photographs of separated children in central locations to support identification.
- Ensure camps or shelters are located as close as possible to affected areas.
- Keep families and community groups together whenever possible.
4.2. Causes of mortality
Mortality in Humanitarian Emergencies
The immediate goal of any intervention in humanitarian emergencies is to reduce the number of deaths. While both conflict and natural disasters can result in immediate deaths, many preventable deaths occur during later phases over a longer period.
Five leading medical problems have consistently been identified as the major causes of mortality in post-conflict or post-natural disaster settings among vulnerable populations (Box 5).
BOX 5. The five leading causes of death in humanitarian emergencies in developing countries
- Diarrheal diseases and dehydration
- Measles
- Malaria
- Acute respiratory infections
- Malnutrition
Unique features in each disaster, such as climate, topography, pre-existing social structure, and physical conditions, affect the proportion of deaths associated with each of these causes, as well as other causes. Figure 7 shows mortality in various displaced populations following natural disasters and armed conflicts.
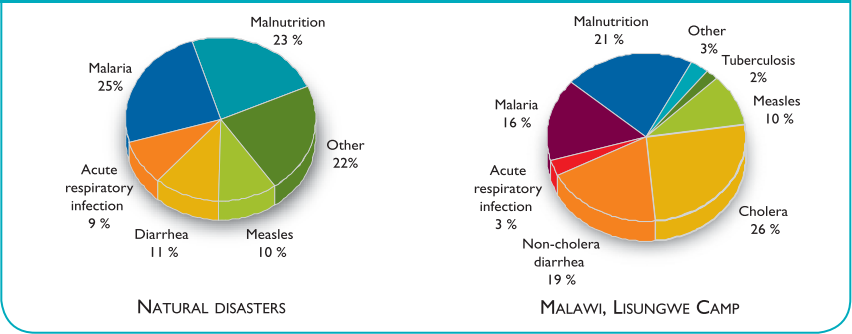
From MMWR, Vol. 41/No. RR-13. Major causes of death in children <5 years old. Source: UNHCR, MSF, IRC monthly report.
Malnutrition, although not identified as a significant immediate cause of death, is the most important factor correlated with high mortality rates due to transmissible diseases. A study including 41 displaced populations (Figure 8) showed a clear correlation between the crude mortality rate (that is, death from all causes) and the prevalence of malnutrition.
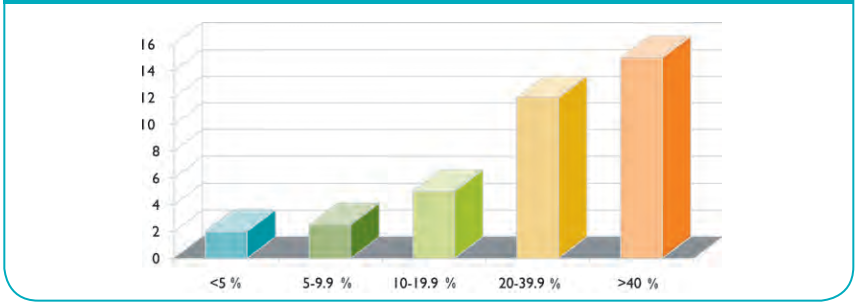
*Malnutrition prevalence in population (%)
(Malnutrition = <80% weight/height WHO reference population)
In the context of a disaster, each of the leading causes of death relates to one or more predisposing environmental conditions that increase the incidence of disease and the mortality rate per case (Box 6). For interventions to be effective, resources should be targeted to prevent and correct these predisposing environmental factors, in addition to treating affected individuals.
BOX 6. Predisposing environmental conditions
- Disruption of food sources/economy
- Disruption of sanitary services
- Income loss
- Discontinuation of healthcare services
- Overcrowding
- Lack of adequate water supply
- Loss of shelter
At a World Health Organization conference, international relief experts identified 10 essential emergency relief measures to consider when planning a disaster response. These interventions should not be implemented in a strict order; the priority of each is correlated with the particular needs of each emergency situation. In addition, these interventions should be adjusted to the specific situation in the affected region.
5. Essential Emergency Relief Measures
OBJECTIVES
- Understand the 10 essential emergency relief measures (as defined by WHO).
- Know how these measures should be implemented in the community.
Emergency Relief Measures
Each disaster or humanitarian emergency is a unique situation determined by the event that caused it, as well as climate, geography, culture, social structure, and the pre-existing conditions of the affected population. Therefore, national and international organizations should begin with a rapid assessment and avoid the impulse to respond immediately before critical information is available.
Interventions based on assumptions rather than accurate, on-site information are likely to waste time and valuable resources, ultimately increasing the suffering of the affected population. Although similar types of disasters have predictable patterns of disruption, as shown in Table 2, the degree of severity and the type of response required are influenced by local conditions.
An appropriate response should be based on the particular needs in each disaster. Needs should be continuously reassessed at local, community, national, and regional levels.
Unanticipated effects may require urgent attention. For example, a safe water supply may not be directly affected by a strong storm or mudslide. However, if the regional system for water pumping or purification is damaged, access to safe water becomes a critical issue that must be addressed to prevent disease and excessive mortality.
Resources must be used in a timely manner within the time frame dictated by the disaster. For example, trauma is often the leading cause of death immediately after an earthquake. If trauma teams and field hospitals arrive a week later, most trauma-related deaths will already have occurred, and the benefit of these high-cost resources will be limited.
WHO and PAHO have developed guidelines for the appropriate use of field hospitals in sudden-impact disasters. More information is available at https://www.paho.org/disasters
5.1. Essential emergency relief measures
Essential Emergency Relief Measures
1. Do a rapid assessment of the emergency situation and the affected population.
An assessment should accurately define needs so that limited resources can be used efficiently to maximize lifesaving and other vital goals.
National level: Assessments are typically carried out by expert teams focused on promptly defining the magnitude of the emergency, environmental conditions, infrastructure damage, the major health and nutrition needs of the affected population, and local response capacity.
Community level: In the immediate aftermath of a disaster, the initial response will primarily come from local resources. Communities must be prepared to carry out a local assessment of disaster impact. Healthcare professionals should be prepared to assess health issues in their community and understand how to share that information with higher levels of authority in order to contribute to regional or national assessments. Assessments need to be repeated, and the quality and specificity of data should be improved during the rescue and recovery phases or whenever any major change occurs, such as an aftershock. Information gathered through assessments is used by resource managers to determine the allocation of resources in any large-scale disaster.
2. Provide adequate shelter and clothing.
Exposure to climatic conditions in disaster situations can increase caloric requirements and lead to death.
Community level: Find short-term shelter for all homeless individuals, particularly vulnerable populations. Shelters should be appropriate for the climate. Keep individuals within their communities and family networks as much as possible. In general, it is recommended that resources be directed to rebuilding within the community rather than to building large camps or temporary settlements outside the disaster area.
3. Provide adequate nutrition.
Large-scale bulk food requirements are typically calculated based on a minimum of 2,100 kcal per person per day.
Large-scale bulk food requirements are typically calculated based on a minimum of 2,100 kcal/person/day.
Community level: Communities must plan to distribute food equitably and include vulnerable groups. As food resources improve, establish targeted supplemental and therapeutic feeding programs for malnourished individuals.
4. Provide elementary sanitation and clean water.
The estimated minimum requirement for drinking water is 3-5 L per person per day of clean water, but 15-20 L per person per day are recommended for all needs, including washing and cooking.
Community level: Re-establish supplies of clean water and effective sanitation and waste disposal services as soon as possible. In an emergency, there should be at least one latrine for every 20 individuals. As the situation stabilizes, each family of five should have one latrine.
5. Set up a diarrhea control program.
An increase in diarrheal disease is a predictable outcome of disasters because of disruption to infrastructure and healthcare services.
Community level: Rapidly implement community-based education on appropriate household sanitation measures, diarrhea prevention, and household case management, particularly for young children with diarrhea. Healthcare centers should anticipate additional cases of dehydration, use appropriate low-cost strategies such as ORS/ORT, and recognize possible cases of cholera and dysentery.
Many casualties can largely be prevented by community health education and access to appropriate primary care for treatment.
6. Immunize against measles and provide vitamin A supplements.
Measles has been a major source of mortality among crowded, displaced populations in which malnutrition is prevalent. Therefore, measles immunization is the only vaccine that is routinely considered for use as a preventive measure immediately following a disaster. Since vitamin A deficiency is common and contributes to measles-related mortality, consider mass distribution of vitamin A for vulnerable populations.
National level: National and international agencies work together to determine if measles immunization or vitamin A distribution is necessary following a particular event. If necessary for all or part of the deemed population, national authorities establish the central logistics (e.g., cold chain, personnel, materials) to manage a mass immunization/distribution campaign.
Community level: Health officers must immediately assess the available cold chain as part of its health care assessment. Health care professionals must monitor for cases of measles and develop a plan for mass immunization and/or mass distribution of vitamin A to the vulnerable groups in their community.
7. Establish minimum reproductive health and HIV services and improve primary medical care.
Immediate casualties (rescue phase) of a sudden impact disaster are likely to include a limited number of trauma victims. In most disasters in fragile communities the larger number of disaster-related deaths (i.e., deaths above the baseline crude mortality rate) will be due to preventable causes of mortality in the weeks and months following the impact. These casualties can largely be prevented by community health education and access to appropriate primary care. This included emergency obstetric and neonatal care, prevention and management of sexually transmitted infections, management of the health effects of sexual violence, ensuring safe blood transfusion and universal precautions in health facilities. Initial efforts should be focused on identifying those who were on treatment before the onset of the disaster and to restart treatment for them.
Community level: Health professionals should know the emergency transport and response systems in their community. Health care interventions during the rescue phase should include minimizing life losses caused by the direct impact of the event (e.g., trauma, drowning). After the rescue phase, health care resources should be focused on re-establishing and improving the access and quality of primary care, particularly for the most vulnerable groups.
8. Set up disease surveillance and health information systems.
Effective health information and disease surveillance systems are necessary to monitor effectiveness of health interventions and reassign priorities.
National level: Health authorities will use available information to define initial priorities in the use of limited resources. They should develop specific surveillance guidelines for each disaster in order to track relevant disease/mortality trends.
Community level: Every health care delivery setting should immediately implement a simple but effective health information collection system based on established WHO, PAHO, or governmental guidelines. Health care professionals should know how to share this information regularly with higher level health authorities.
9. Organize human resources.
The initial shock of an event can make it difficult for a disaster-affected population to effectively respond in a quick and organized fashion. Having a pre-defined emergency plan with clearly-identified leaders can help the local community to cope until more external resources arrive.
Community level: Have an emergency plan and pre-defined community leaders for:
- Conducting rescue operations
- Conducting assessments (e.g., health services, transportation, food, sanitation/water systems)
- Organization of food and water distribution, and the sanitary program
- Health services management
- Corpses and gravesite management
- Identification of unaccompanied minors or other extremely vulnerable individuals (e.g., elderly or persons with a disability) and organization of a caregiver program.
10. Coordinate activities.
National level: In a large-scale disaster there will be many national and international agencies attempting to assess, develop plans, and establish priorities for funding at national and regional levels. Most effective relief efforts have resulted from effective collaboration between many agencies, each bringing their own expertise and experience. However, all of these agencies will ultimately depend on quality assessments from the affected communities to make appropriate decisions and determine the ability of the communities to implement the plans and projects that will help diminish suffering and restore the baseline situation in the communities.
Community level: Develop local emergency plans that link into regional and national plans and agencies. Understand the mechanisms for communication of information (e.g., assessments, surveillance data) during disasters. Build relationships with key individuals within and outside the community before a disaster occurs.
6. Organizations
OBJECTIVES
- Identify national and international organizations that may respond to a humanitarian emergency in your country.
- Recognize the available resources, strengths, and limitations of these organizations.
Organizations capable of providing assistance during humanitarian emergencies
When local resources are insufficient, assistance from multiple national or perhaps multinational organizations will be needed. Each involved organization has its own institutional structure and culture, in addition to other features, such as capacity for response, technical and logistic resources, and thematic or regional approach.
Several international agencies may have activities in the country prior to the event. In response to the disaster these agencies may retarget their resources in the country to emergency relief. Effective coordination and cooperation among involved organizations are essential but very difficult to achieve in the chaotic situation of a massive emergency. There are two major types of organizations that can get involved in assistance when a disaster
National departments - These are agencies at the national level that have authority for disaster planning and response. A regional conference on disasters took place in 1986 to optimize the preparedness and response mechanisms of Latin American and Caribbean nations. As a result of this conference, most nations established a health disaster coordinator. The health disaster coordinator not only coordinates health-related relief efforts in the event of a disaster, but also continuously updates emergency plans and conducts preparedness training for health care professionals.
Pan American Health Organization (PAHO) - This is an international public health agency serving as the Regional Office for the Americas of the World Health Organization. It provides health policy guidance and technical assistance in disaster planning and response (Box 7). More information is available at: www.paho.org.
BOX 7. Some technical recommendations for disaster situations issued by the PAHO
- Specific topics related to disasters
- For example, frequent effects of specific types of disasters, such as volcanic eruptions.
- Special needs
- Special considerations regarding vulnerable groups.
- Transmissible diseases
- Vector control; specific behaviors for cholera and tuberculosis in the context of disasters.
- Food safety
- Guidelines for food preparation and nutrition.
- Immunization
- For example, the adequate use of measles and equine encephalitis vaccines in the context of disasters.
- Environmental sanitation
- Rodent prevention; general health recommendations for camps and shelters; guidelines for temporary shelters.
Source: www.paho.org
World Health Organization (WHO)—The WHO provides technical advice and develops health policies relating to disasters. More information is available at: www.who.int.
SUMA (Humanitarian Supply Administration System, developed by the PAHO) - This organization facilitates the reception, inventory, and rapid distribution of essential humanitarian supplies and equipment. In the event of a disaster, PAHO can send SUMA-trained staff to the affected country to assist in managing the inflow of supplies.
United Nations (UN) - The UN is a multinational organization that functions mainly through its sub-agencies, which are independently funded. More information is available at: www.un.org.
The Office of the United Nations High Commissioner for Refugees (UNHCR) - The agency is mandated to lead and coordinate international action to protect refugees and resolve refugee problems worldwide. Its primary purpose is to safeguard the rights and well being of refugees. It strives to ensure everyone can exercise the right to seek asylum and find safe refuge in another State, with the option to return home voluntarily, integrate locally, or to resettle in a third country. More information is available at: www.unhcr.org.
World Food Program (WFP) - This organization coordinates the delivery of food to regions in need around the world. More information available at: www.wfp.org.
United Nations International Children’s Emergency Fund (UNICEF) This organization was created by the UN General Assembly to advocate and protect children’s rights, to help fulfill their basic needs, and to provide opportunities for maximizing the development of their potential. When an emergency occurs, UNICEF focuses on ensuring that basic needs of women and children are fulfilled and on protecting their basic rights. More information is available at: www.unicef.org.
Office for the Coordination of Humanitarian Affairs (OCHA)—In 1998 the OCHA resulted from the reorganization of the UN Department of Humanitarian Affairs (DHA). Its mission was expanded to include the coordination of humanitarian response, policy development, and advocacy. OCHA’s tasks are done through the Inter Agency Permanent Committee that includes multiple participating organizations, such as UN agencies, funds, and programs, the Red Cross, and NGOs. More information is available at: www.unocha.org.
Foreign organizations that provide help in case of disaster
Foreign organizations that provide help in case of disaster - Box 8 identifies some of the governmental agencies of developed countries that provide funding and technical help to countries affected by humanitarian emergencies. PAHO and WHO have developed guidelines to assist disaster-affected countries in managing donor offers from various agencies. According to the 1999 PAHO publication Humanitarian Assistance in Disaster Situations: A Guide for Effective Aid, “In the most advanced developing countries, in particular in Latin America, national health services, voluntary organizations and the affected communities mobilize their own resources to meet the most compelling medical needs in the early phase after a disaster. Requirements for external assistance are generally limited to highly skilled expertise or equipment in a few specialized areas.”
BOX 8. Foreign agencies for disaster assistance
Military help
Military help - Both local and foreign military can be mobilized to assist in the response to natural disasters or complex emergencies. Certain unique features make military organizations useful in a disaster.
6.1. Advantages
Military Help
Speed: Few organizations are capable of implementing a large logistic response as rapidly as the military.
Security: The military can secure a specified environment, population, and material.
Transportation: Their fleet of planes and helicopters, as well as land and naval equipment, enable them to transport resources readily.
Logistics: They have experience in maintaining supply lines in problematic environments and situations.
Command, control, and communication: They have a well-defined and responsive organizational structure.
Self-sufficiency in the field: When military arrive to the region where the event has occurred, they are capable of fulfilling the needs of their own personnel.
Specialized units: They often have specifically trained and equipped units. These include engineers who can provide technical assistance and preventive medicine teams capable of rapidly performing epidemiologic evaluations and surveillance, outbreak investigations, vector control, and water purification and treatment.
Field hospitals and capacity for medical evacuation: Hospitals can be helpful in certain circumstances. See the WHO-PAHO guidelines for the use of field hospitals in sudden-impact disasters.
6.2. Shortcomings
Limitations of Military Assistance
Despite all the advantages mentioned above, the use of the military can have significant shortcomings and limitations in some situations.
Medical care: Field hospitals are designed for the care of soldiers wounded in combat (i.e., for the care of wounds suffered by healthy adults). During a disaster, primary care and preventive interventions for women and children are major needs.
Logistics: Supplies available in the military response system may not be appropriate for a disaster in terms of prevailing diseases or types of food.
Political objectives: The military are an asset of governments; in addition, certain humanitarian objectives can be subordinated to other political or strategic goals. The presence of the army in certain scenarios can cause tension in certain groups of the population and compromise relief workers who, for their own safety and function, wish to be considered neutral.
Cost: Military activities are expensive.
7. Nongovernmental organizations
Non-Governmental Organizations
NGOs are nonprofit organizations working on a full-time basis in assistance for appropriate development. Thousands of NGOs, both international and national, are functioning throughout the world. Most NGOs are small agencies focusing on very specific development projects (e.g., providing education, working tools, or training in sustainable development). Only a few of them have the resources required for supporting activities targeted to promote development and to respond to disasters in multiple countries or regions. Each NGO is specialized in specific aspects of assistance in emergencies (Box 9). Although NGOs may receive contributions from individuals, most of their funds come from the governments of industrialized countries. These governments distribute their money for assisting projects through contracts with NGOs. Unlike the International Committee of the Red Cross (ICRC), some NGOs maintain a “right to interfere.” This means they can operate across borders without written approval of their hosts.
BOX 9. Most important NGOs and their specialization fields
| Organization | Specialization field | Website |
|---|---|---|
| Action Contre La Faim | Prevention, detection and treatment of malnutrition | http://www.actioncontrelafaim.org/en |
| Catholic Relief Services | Food distribution | www.crs.org |
| Cooperative for the American Relief Everywhere (CARE) | Assistance in logistics and feeding; camp management | www.care.org |
| International Medical Corps | Health care training, relief and development programs | www.internationalmedicalcorps.org |
| International Rescue Committe | Medical care | www.theirc.org |
| Irish Concern | Feeding supplementation | |
| Médecins sans Frontières | Medical care | https://www.msf.org |
| Medicins Du Monde | Emergency relief and advocacy | www.medicinsdumonde.org |
| Oxford Committee for Famine Relief (OXFAM) | Water and sanitary services | www.oxfam.org.uk |
| Plan International | Child health and development | www.plan-international.org |
| Save the Children Fund | Assistance in feeding and development | www.savethechildren.org.uk |
| World Vision | Assistance in feeding and development | www.worldvision.org |
Although usually looking for the neutrality of the ICRC, some NGOs may be more willing to report any perceived injustice. They perform well in emergencies within their area of specialty (e.g., water provision, food distribution), but most cannot achieve self-sufficiency in an emergency setting and rely on UN, military, or other agencies for security, transportation to remote sites, communication, support of logistics, or medical care for their own personnel. NGOs have enhanced ability to provide person-to-person assistance because they are likely to have a pre-disaster relationship with the affected communities and understand the local culture and public health issues. They can also shift easily from disaster relief to development, and are willing to make a long-term commitment to community development and rebuilding.
International Committee of the Red Cross (ICRC)
International Committee of the Red Cross (ICRC)—This is a hybrid agency: neither private nor controlled by a government. A number of its characteristics are unique; its mission is defined by the international humanitarian law passed by the 1949 Geneva Convention and the two 1977 protocols. The ICRC gets involved mainly when civil disturbances are present; it has the right and duty to intervene across borders when national or international conflicts break out, regardless of whether a “state of war” has been declared. The ICRC brokers relief assistance during war, assures legal protection for victims, and monitors the way Prisoners of War are managed. Also, the ICRC plays a critical role in reuniting families. The ICRC strives to preserve its neutrality, which is essential for its mission and enables its members to work unarmed in war regions under the control of any of the involved parties.
The ICRC provides a complete account of its activities to all the parties involved in the conflict. It will refuse to participate in any activity that can be seen as showing favoritism. This may include transportation in vehicles belonging to one of the parties or joining efforts with groups that have their own interests. The ICRC is usually self-sufficient and can use its own resources for air lifts, communication, and logistics. It will participate only if all parties involved in the conflict sign an agreement recognizing and showing respect for its neutrality and mission. The ICRC is related to but independent from the Red Cross and the Red Crescent Societies national agencies. These organizations provide assistance primarily to victims of disasters or wars within their own nations. They have a similar commitment with neutrality, provision of assistance based only on the need, and independence from national governments.
7.1. Coordination of organizations
Coordinating Disaster Response Activities
Coordinating the activities of all these organizations poses a tremendous challenge. Following a natural disaster the host nation’s government/agencies and military are likely to have operational command. Most nations now have defined governmental authorities responsible for global disaster planning and response, as well as coordinators for individual sectors such as health. External agencies or governments play a supportive role in providing technical assistance and resources. PAHO has developed a number of technical manuals and training activities to assist nations in the planning of coordinated disaster responses at the regional and national level.
In complex emergencies related to a conflict, the armed forces or government authorities will have the command of operations, including the coordination of humanitarian help. The coordination in this scenario can be particularly difficult if the hostile groups are stationed nearby and try to block assistance of civilians. In this context, humanitarian help can be used as a political and strategic instrument.
Medical Volunteering
Following a disaster many pediatricians and other health professionals volunteer for a limited time. During the initial response phase, the greatest pediatric needs include air transport teams, surgical teams (a surgeon, OR nurse, anesthesiologist, and critical care pediatrician), as well as pediatricians with training and experience in emergency medicine and critical care. Volunteers may have to be self sufficient for a period of time in terms of food, water, and shelter. Volunteers should work through an established NGO or governmental agency rather than simply “show up” to help. Volunteers should be prepared to respond quickly, as the quicker the response teams can provide appropriate care, the more effective they can be at saving lives and limiting morbidity.

It is critical to attempt to reunite children with their families as soon as possible and pay special attention to reducing their vulnerability in all disaster response planning.
Part of preparation is anticipating the types of injuries that will be seen with different types of disasters. When sending a response team into a disaster during the acute response phase, it is important to have the personnel with the ability to treat the most likely injuries seen with the specific type of disaster. In a major earthquake like the one in Haiti in January 2010, one would expect the majority of the casualties to be secondary to traumatic injuries related to collapsed buildings.
Therefore, a team should be prepared to have personnel and supplies that can be used to treat crush injuries, a large number of open wounds, along with a variety of orthopedic injuries. In a disaster involving an explosion (large industrial accident or terrorist attack), the pattern of injuries would include many of the same traumatic injuries as seen in an earthquake, but would also include a large number of burns and blast injuries such as blast lung. Personnel required in this type of disaster should include those with training in caring for burns as well as experience with other traumatic injuries.
In the first days following the Haiti earthquake, there were a large number of complex orthopedic injuries that required emergent treatment. These included open fractures, traumatic amputations, and crush injuries. The treatment of these injuries included fracture reductions, wound debridement, and amputations. Thus it was essential to have personnel with the training to perform the needed procedures. Personnel with training in emergency medicine, general surgery, and orthopedics are best suited to be part of the initial response team when a large number of traumatic injuries are expected.
Supplies that are essential in caring for these patients include plaster splinting/casting supplies, wound dressing supplies, and medications for pain control and sedation. When caring for open wounds, the ability to appropriately irrigate and clean wounds can greatly reduce subsequent secondary infections of these wounds. Response teams should come prepared with supplies that would be able to provide pressure irrigation of wounds with either clean water or saline, antibiotic ointments, and large supplies of wound dressings. A large number of the orthopedic injuries can be treated with casting or splinting. Plaster casting material is far superior in this setting since casts made of fiberglass cannot be easily removed without a cast saw, whereas patients/families can be instructed to remove a plaster cast by soaking it in water.
Table 4 provides a list of pediatric equipment that, if possible, should be brought in if not available on site.
TABLE 4. Recommended equipment to bring for pediatric emergencies in disaster situations.
Airway Management/Breathing
- Tongue Blades
- Suctioning machine (portable, battery-powered)
- Suction catheters -Yankauer, 8, 10, 14F
- Simple face masks - infant, child, adult
- Pediatric and adult masks for assisted ventilation
- Self-inflating bag with 250 cc, 500 cc, and 1000 cc reservoir
Optional for intubation
- Laryngoscope handle with batteries (extra batteries AA, laryngoscope bulbs)
- Miller blades - 0, 1,2,3 Macintosh blades 2,3
- Endotracheal tubes, uncuffed - 3.0, 3.5, 4.0,4.5, 5.0, 6.0, cuffed - 7.0,8.0
- Laryngeal mask airways
- Stylets - small, large
- Easycap (ETCO2 analyzer), 2 sizes
- Adhesive tape to secure ETT
Circulation/Intravascular Access or Fluid Management
- IV catheters - 18-, 20-, 22-, 24-gauge
- Butterfly needles - 23-gauge
- Intraosseous needles- 15- or 18-gauge, or Eazy IO device
- Boards, tape, tourniquet IV
- Pediatric drip chambers and tubing
- 5% dextrose in normal saline and half normal saline
- Isotonic fluids (normal saline or lactated Ringer’s solution)
- Medications: epinephrine, atropine, sodium bicarbonate, calcium chloride, lidocaine, D25, D10
Miscellaneous
- Broselow tape
- Nasogastric tubes - 8, 10, 14F
- Splints and gauze padding
- Rolling carts with supplies such as abundant blankets
- Warm water source and portable showers for decontamination
- Thermal control (radiant cradle, lamps)
- Geiger counter (if suspicion of radioactive contamination)
- Personal protective equipment (PPE)
- Pain/Sedation medications: ketamine, morphine, ketorolac
- Other potential medications: albuterol, cephalexin, cefazolin, ceftriaxone, diazepam
- Surgical equipment for amputations, incision and drainage of wounds, laceration repairs
- Headlamps with replacement batteries
- Scissors
- Plaster for casting, not fiberglass (hard to remove)
Monitoring Equipment
- Sphygmomanometer/ Blood pressure cuffs - premature, infant, child, adult
- Portable monitor/defibrillator (with settings < 10)
- Pediatric defibrillation paddles
- Pediatric electrocardiogram (ECG) skin electrode contacts (peel and stick)
- Pulse oxymeter with reusable (older children) and nonreusable (small children) sensors
- Device to check serum glucose and strips to check urine for glucose, blood, etc.
Among the recommended equipment, elements for proper airway management in children are crucial. A major challenge of any disaster response is gathering, organizing, and moving supplies to the affected area. Resource management within the hospital and other facilities or agencies may prove to be a decisive factor in whether a mass casualty event can be handled.
Communication
Communication in a disaster situation is essential between disaster relief team members as well as with coordinating groups and logistical support personnel in home countries. Modern technology has provided many different types of communication devices, which have different advantages and disadvantages. Communication networks and contingency plans are an essential part of the disaster preparedness phase. Radios are useful for short range communications when a disaster relief team is separated. However, they are limited by range and will not allow communication with the other teams or organizations that are a long distance away.
Satellite phones are ideal for communication with the team as well as with the home country. They provide a reliable method of communication when telephone services are not working or there is no infrastructure, because they rely on orbiting satellites to transmit data. However, they are a scarce resource as well as an expensive resource. The main drawback for many portable satellite phones is that the phone’s antenna needs an unobstructed view of the sky.
Cellular phones are an ideal method for communication. Voice calls can be made to team members as well as to coordinate in the home country. E-mail and SMS texting are other methods of communicating through the cellular network. However, cellular technology is dependent on a cellular infrastructure and network that has survived a disaster. The cellular networks may also become overwhelmed by the number of people attempting to use it in the time after the disaster, thus emergency/disaster relief providers and organizations need to have a communication system that is reliable and free of interference.
The availability of the internet through various means including satellite links and data over cellular networks has allowed for many novel methods of communication over the internet. There are traditional methods such as electronic mail. Web blogs also allow relief workers as well as those affected by the disaster to reach out to the world. Other social media tools such as Facebook and the microblogging service Twitter allow almost instantaneous updates from the field.
Mental health considerations
Disaster response providers are often thrust in to a high stress situation with exposure to situations they may have never experienced before. The degree of destruction and death will likely be much greater than what the health care providers are accustomed to dealing with in their daily lives. Local first responders and medical providers thrust in to the role of the initial emergency response phase may be faced with the additional stress of personally knowing many of the victims (or their family members) that they are caring for.
The emotional impact of large scale destruction, suffering, and death will elicit different responses in different people, but all volunteer providers should recognize how their experiences can affect their wellbeing both emotionally and physically. The emotional stress experienced by disaster response providers has been well documented after events such as 9/11 and Hurricane Katrina. The effect of stress is amplified by the long hours of intense work experienced during the response to a disaster. Environmental conditions (such as extreme heat/cold/rain/flooding), lack of sleep, and inadequate nutrition impair a provider’s ability to deal with the stressful situation.
Crisis response workers and managers, including first responders, public health workers, construction workers, transportation workers, utilities workers and other volunteers, are repeatedly exposed to extraordinarily stressful events. This places them at higher than normal risk for developing stress reactions (Pan American Health Organization [PAHO], 2001). It is important for all disaster response providers to recognize the potential emotional stress they will be entering before arriving on scene. Stress prevention and management needs to be considered and addressed from the start of the deployment in order to prevent problems. By anticipating stressors and individual's responses to these stressors, the response team and individuals can potentially prevent a crisis within the team of care providers.
The US Department of Health and Human Service, Substance Abuse and Mental Health Services Administration (SAMHSA), and Center for Mental Health Services (CMHS) have published a guide focusing on general principles of stress management and offers simple, practical strategies that can be incorporated into the daily routine of managers and workers. It also provides a concise orientation to the signs and symptoms of stress.
While most people are resilient, the stress response becomes problematic when it does not or cannot turn off, that is, when symptoms last too long or interfere with daily life. Table 5 provides a list of the common stress reactions.
TABLE 5. Common Stress Reactions
Behavioral
- Increase or decrease in activity level
- Substance use or abuse (alcohol or drugs)
- Difficulty communicating or listening
- Irritability, outbursts of anger, frequent arguments
- Inability to rest or relax
- Decline in job performance; absenteeism
- Frequent crying
- Hyper-vigilance or excessive worry
- Avoidance of activities or places that trigger memories
- Becoming accident prone
Physical
- Gastrointestinal problems
- Headaches, other aches and pains
- Visual disturbances
- Weight loss or gain
- Sweating or chills
- Tremors or muscle twitching
- Being easily startled
- Chronic fatigue or sleep disturbances
- Immune system disorders
Psychological/Emotional
- Feeling heroic, euphoric, or invulnerable
- Denial
- Anxiety or fear
- Depression
- Guilt
- Apathy
- Grief
Thinking
- Memory problems
- Disorientation and confusion
- Slow thought processes; lack of concentration
- Difficulty setting priorities or making decisions
- Loss of objectivity
Social
- Isolation
- Blaming
- Difficulty in giving or accepting support or help
- Inability to experience pleasure or have fun
8. Conclusion
Conclusion
Disasters are, to a great extent, beyond our control and inevitable. However, we can be better prepared for the consequences and thus reduce the degree of human suffering.
“Experience is a hard teacher. She gives the test first and the lessons afterwards.”
As Vernon Law has said, “Experience is a hard teacher. She gives the test first and the lessons afterwards.” Knowledge and understanding are needed for more effective preparation and planning.
Pediatricians have a special role in the planning and preparation process to ensure that the needs of children are adequately considered in this process.
Pediatric volunteers should be prepared for their experiences from the standpoint of training, available materials and resources, and mental health considerations.
9. Suggested Reading
References
- Bhave S, Mathur Y, Agarwal V, eds. Guidelines on the Management of Children in Disaster Affected Situations. Indian Academy of Pediatrics, 2005.
- Burkholder B, Toole M. Evolution of Complex Disasters. Lancet 1995;346:1012.
- Burkle FM. Complex Humanitarian Emergencies: I. Concept and Participants. Prehospital and Disaster Medicine 1995;10:48-56
- Davidson LW, Hayes MD, Landon J. Humanitarian and Peace Operations: NGOs and the Military in the Interagency Process. Workshop Report, 1996. National Defense University Press, Washington DC.
- CDC Famine-Affected, Refugee and Displaced Populations: Recommendations for Public Health Issues. CDC, MMWR 1992;41:RR-13.
- Gaydos J, Luz G. Military Participation in Emergency Humanitarian Assistance. Disasters 1994;18:48.
- Handbook of War and Public Health, ICRC, Geneve, 1996
- Leaning J, Briggs S, Chen L, eds. Humanitarian Crises: The Medical and Public Health Response. Harvard University Press, Cambridge, MA, 1999.
- Levy B, Sidel V, ed. War and Public Health. Oxford University Press, New York 1997.
- Lillibridge SR, Burkle F, Noji E. Disaster Mitigation and Humanitarian Assistance Training for Uniformed Services Medical Personnel. Military Medicine 1994;159:397.
- Marks E. Complex Emergencies: Bureaucratic Arrangements in the UN Secretariat. National Defense University Press, Washington DC, 1996
- Mothershead JL, et al. Disaster Planning. Available at: http://www.emedicine.com/emerg/topic718.htm.
- Noji E. K. The Public Health Consequences of Disasters, Oxford University Press, 1997
- Sandler R, Jones T, eds. Medical Care of Refugees. Oxford University Press, New York, 1987.
- Mandalakas A, Torjesen K, Olness K, eds. Helping the Children: A Practical Handbook for Complex Humanitarian Emergencies. Johnson and Johnson Pediatric Institute and Health Frontiers, Kenyon, MN, 1999.
- Romig LE. Disaster Management. In: APLS Course Manual. Jones & Bartlett Publishers, 2006.
- Sharp TW. Conflict-Related Complex Emergencies, in Chap. 34, Military Preventive Medicine, 1997.
- Sharp TW. The Challenge of Humanitarian Assistance in the Aftermath of Disasters Chap. 32, Military Preventive Medicine, 1997.
- Sharp T, Yip R, Malone JD. US Military Forces and Emergency International Humanitarian Assistance-Observations and Recommendations from Three Recent Missions. JAMA 1994;272:386.
- Toole MJ. Mass Population Displacement-A Global Public Health Challenge. Infectious Disease Clinics of North America 1995;9:353.
- Walker P. Foreign Military Resources for Disaster Relief: an NGO Perspective. Disasters 2005;16:152.
- http://www.reliefweb.int/rw/rwb.nsf/db900sid/EGUA-836R39?OpenDocument&RSS20&RSS20=FS
http://www.google.com/hostednews/afp/article/ALeqM5hOiPk5G7TMLjYsBbZ1ajaBMS_lWg
or
http://www.reliefweb.int/rw/rwb.nsf/db900sid/SNAA-82587M?OpenDocument&rc=2&emid=EQ-2010-000009-HTI
http://www.nytimes.com/2010/02/13/world/americas/13doctors.html?hp. - Merin O, Ash N, Levy G, et al. The Israeli Field Hospital in Haiti
- - EthicalDilemmas in Early Disaster Response [in Spanish]. N Engl J Med 2010 0:NEJMp1001693 Observations from Ground Zero at the World Trade Center in New YorkCity, Part I.
- Levenson RL Jr, Acosta JK. Int J Emerg Ment Health. 2001Fall;3(4):241-4. Mental health status of World Trade Center rescue and recovery workers and volunteers - New York City, July 2002-August 2004 [in Spanish].
- Centers for Disease Control and Prevention (CDC). MMWR Morb Mortal Wkly Rep. 2004 Sep 10;53(35):812-5. Mental health of workers and volunteers responding to events of 9/11:review of the literature.
- Bills CB, Levy NA, Sharma V, Charney DS, Herbert R, Moline J, Katz CL. Title? [in Spanish]. Mt Sinai J Med. 2008 Mar-Apr;75(2):115-27.
- Palm KM, Polusny MA, Follette VM. Vicarious traumatization: potential hazards and interventions for disaster and trauma workers. Prehosp Disaster Med. 2004 Jan-Mar;19(1):73-8.
- Pan American Health Organization. (2001). Stress management in disasters. Washington, DC: Pan American Health
10. Case Resolution
Case Discussion
A disaster can be defined as a usually sudden event causing damages, affecting many people, and because of its magnitude, exceeding the capacity for response of local or national organizations. High morbidity and mortality rates are frequently found in the affected population, which is often exposed to critical sanitary situations, both immediately after the disaster and during subsequent phases. There is an additional risk for diseases associated with crowding and lack of adequate public services.
Disasters can be due to natural causes, such as hurricanes and earthquakes, to alterations or to technological causes; i.e., related to events triggered by man’s intervention (e.g., the release of toxic or radioactive agents). In addition, civil or international wars cause complex emergencies that affect civilians and result in their displacement.
In this case, flooding has brought about a natural disaster.
Vulnerable Populations
Children, as well as old people and pregnant women are the most vulnerable populations when a disaster occurs. For children, the risk of being separated from their families determines their vulnerability. In addition, their physical, physiological and mental features render them more susceptible to environmental, sanitary and social changes resulting from disasters.
All affected children should be identified and their identity should be properly documented. They should also receive preferential attention during the distribution of sanitary and feeding resources, as well as effective preventive interventions.
Initial Assessment and Response
The initial and highly critical step is the immediate assessment of the situation and the affected population. This will define the actual needs and the interventions that are most appropriate in the current circumstances. It is important to establish clearly defined priorities and the effective coordination of rescue activities, in both the early and the subsequent phases.
In this case, field hospitals are unlikely to be needed, since traumatized victims requiring immediate interventions will be less numerous than in other circumstances, when disasters have a more sudden and unexpected start.
The capacity for response of local and regional services will determine whether or not external assistance is needed. Immediate external help is unlikely to be necessary in this case, but there will probably be a need for resources to provide the affected population with shelter and clothing.
11. Myths and realities of disasters
Myths and realities of disasters
The Pan American Health Organization has identified many myths and erroneous beliefs that are widely associated with the public health impact of disasters; all disaster planners and managers should be familiar with them.
| MYTH | REALITY |
|---|---|
| Outside medical volunteers with extensive medical training are needed. | The local population almost always covers immediate lifesaving needs. Only medical personnel with skills that are not available in the affected country may be needed. |
| Any kind of outside assistance is needed, and it is needed now! | A hasty response not based on an impartial assessment only contributes to chaos. It is better to wait until real needs have been assessed. As a matter of fact, most needs are met by victims themselves and their local government and agencies, not by outside parties. |
| Epidemics and plagues are inevitable after every disaster. | Epidemics do not spontaneously occur after a disaster, and dead bodies will not lead to catastrophic outbreaks of exotic diseases. The key to preventing disease is to improve sanitary conditions and educate the affected population. |
| Disasters bring out the worst in human behavior (e.g., looting, rioting). | Although isolated cases of antisocial behavior exist, most people respond spontaneously and generously. |
| The affected population is too shocked and helpless to take responsibility for its own survival. | On the contrary, many people find new strength during an emergency, as evidenced by the thousands of volunteers who spontaneously united to sift through the rubble in search of victims after the 1985 Mexico City earthquake. |
| Disasters are random killers. | Disasters strike hardest on more vulnerable groups: the poor, and especially women, children and the elderly. |
| Locating disaster victims in temporary settlements is the best alternative. | It should be the last alternative. Many agencies use funds normally spent for tents to purchase building materials, tools, and other construction-related support in the affected country. |
| Food aid is always required for natural disasters. | Natural disasters only rarely cause loss of crops. Therefore, victims do not always require massive food aid. |
| Clothing is always needed by the victims of a disaster. | Used clothing is almost never needed; it is often culturally inappropriate, and though accepted by disaster victims, it is almost never worn. |
| Things are back to normal within a few weeks. | The effects of a disaster last a long time. Disaster-affected areas lose much of their financial and material resources in the immediate postimpact phase. Successful relief programs gear their opportunities to the fact that outside interest wanes as needs and shortages become more pressing. |