Preventive Medicine in Humanitarian Emergencies
| Site: | Pediatric Pandemic Network Learn |
| Course: | Preventive Medicine in Humanitarian Emergencies |
| Book: | Preventive Medicine in Humanitarian Emergencies |
| Printed by: | Guest user |
| Date: | Wednesday, July 29, 2026, 5:09 PM |
1. Overview
Welcome to this multimedia open access edition of this chapter book titled Preventive Medicine in Humanitarian Emergencies.

This content is available as a digital book in two formats:
1) Website, which you are currently reading. This format offers a mobile friendly multimedia experience with sharable links to chapters. There are three ways to move through the book:
a) Use the table of contents chapter navigation to the left to navigate to different chapters in the book. Scroll through the links to select the chapter that interests you.
b) Use the yellow arrows that appear when scrolling to select previous and next chapters.
c) Use the previous chapter and next chapter buttons at the bottom of very page to navigate through the book.
2) Printable, which you can save as a PDF and open without an Internet connection.
1.1. Acknowledgements
Created by the Center for Global Health, Colorado School of Public Health
This content is owned by the Center for Global Health, Colorado School of Public Health, and has been jointly created by the Center for Global Health, Colorado School of Public Health and the Maternal and Child Health Department of Maimonides University; both of which are WHO Collaborating Centers in Maternal and Child Health. The course materials were developed with input from the American Academy of Pediatrics (AAP), the Pan American Health Organization (PAHO), and the Association for Health Research & Development (ACINDES).
With Support from the Pediatric Pandemic Network

The Pediatric Pandemic Network is supported in part by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) as part of cooperative agreements U1IMC43532 and U1IMC45814 with 0 percent financed with nongovernmental sources. The content presented here is that of the authors and does not necessarily represent the official views of, nor an endorsement by HRSA, HHS, or the U.S. Government. For more information, visit HRSA.gov.
Attribution-NonCommercial-NoDerivatives CC BY-NC-ND
You are free to download and share this work for noncommercial purposes, as long as you credit the Center for Global Health and the Pediatric Pandemic Network for the original creation.
2. Introduction
Book Authors
Douglas A. Lougee, MD, MPH
Sathyanarayanan Doraiswamy
Dr. Ángela Gentile
Why is Preventive Medicine and Public Health Important after a Disaster?
In a post-disaster scenario, health workers are faced with many challenges. For example, they may be concerned for the safety and well-being of their own families as well as the health and well-being of their patients. Most will have an innate desire to help their community. Depending on the specific scenario, pediatricians may have to use skills that are beyond those of everyday practice, such as trauma care in the immediate aftermath of an earthquake. However, in any disaster situation, preventive medicine and public health techniques are likely to be most useful aspects for overall community recovery.
At its core, preventive medicine focuses on the use of population health data and public health strategies to improve the health of an entire community. After a disaster, the day-to-day public health infrastructure is suddenly disrupted. Much like the autonomic nervous system, which maintains bodily functions without conscious effort, this infrastructure works day and night to maintain community health without being appreciated. Following a sudden disruption of the public health services, the community faces potentially catastrophic consequences of not knowing where to go to seek preventive and treatment services. The collapse of public health systems puts communities at high risk of communicable diseases which are associated with high morbidity and mortality.
In these situations, reestablishing the public health infrastructure should have a higher priority than caring for individual patients.
3. Gathering and Using Data
OBJECTIVES
- Recognize the difference between standard clinical practice and preventive medicine.
- Recall the ways in which, after a disaster, public health measures have a higher priority than caring for individual patients.
- Describe and apply population evaluation tools such as rates and underlying causes of disease present in a given community affected by a disaster.
Preventive Medicine: A Public Health Mindset
In clinical practice, physicians spend most of their time diagnosing and treating patients one at a time. Most health care is focused on caring for the patient. Preventive medicine, rather than trying to help the individual patient, focuses on the underlying causes of illness in society and employs public health techniques to address these problems at the population level (Box 1).
BOX 1: Characteristics of preventive medicine
- It is based on public health
- It deals primarily with the health of groups, not of individuals
- It uses mathematical data
- It investigates the underlying causes of disease in the community
The preventive medicine “patient” is considered a group of people, a population, or an entire community with sub-groups within that community. The first step the transition from clinical practice to preventive medicine is to understand your patient. In clinical practice, patients come for consultation with the clinician one by one. Vital signs are determined, and the history, physical examination, and perhaps laboratory tests are used to arrive at a diagnosis and rational treatment plan.
In preventive medicine, the patient is not an individual but a group of people: an entire community. Arriving at an accurate “community health” diagnosis involves taking “vital signs”; however, in this case, those vital signs are mathematical data —rates —of disease within the community and sub-groups within it.
Rates facilitate the comparison between the reality of one community and that of others. They also help assess through time the success of interventions in a given population.
Read the case and consider your answers. Additional case questions appear in later chapters; answers are provided in Chapter 8, Case Resolution.
CASE
After an earthquake, a food poisoning outbreak was detected in a club used as a shelter. An epidemiologist conducted the investigation. On his arrival, Dr. HN was informed that on the previous night all the affected persons had eaten at the club. The investigation focused on the meals served the previous evening. Seventy-five of the 80 persons who had been present were asked about symptoms, including when they were first noticed (date and time of their onset). There were 46 persons with symptoms of gastroenteritis.
- Can the situation be considered epidemic?
In all cases, the symptoms, primarily nausea, vomiting, diarrhea, and abdominal pain, had an acute onset. None of the persons had fever. They all recovered spontaneously in a 24- to 30-hour period. Approximately 20% of the persons who had dinner at the club sought medical care. Samples for fecal culture were not obtained.
- List the diseases that should be considered in the differential diagnosis when an outbreak of acute gastroenteritis occurs.
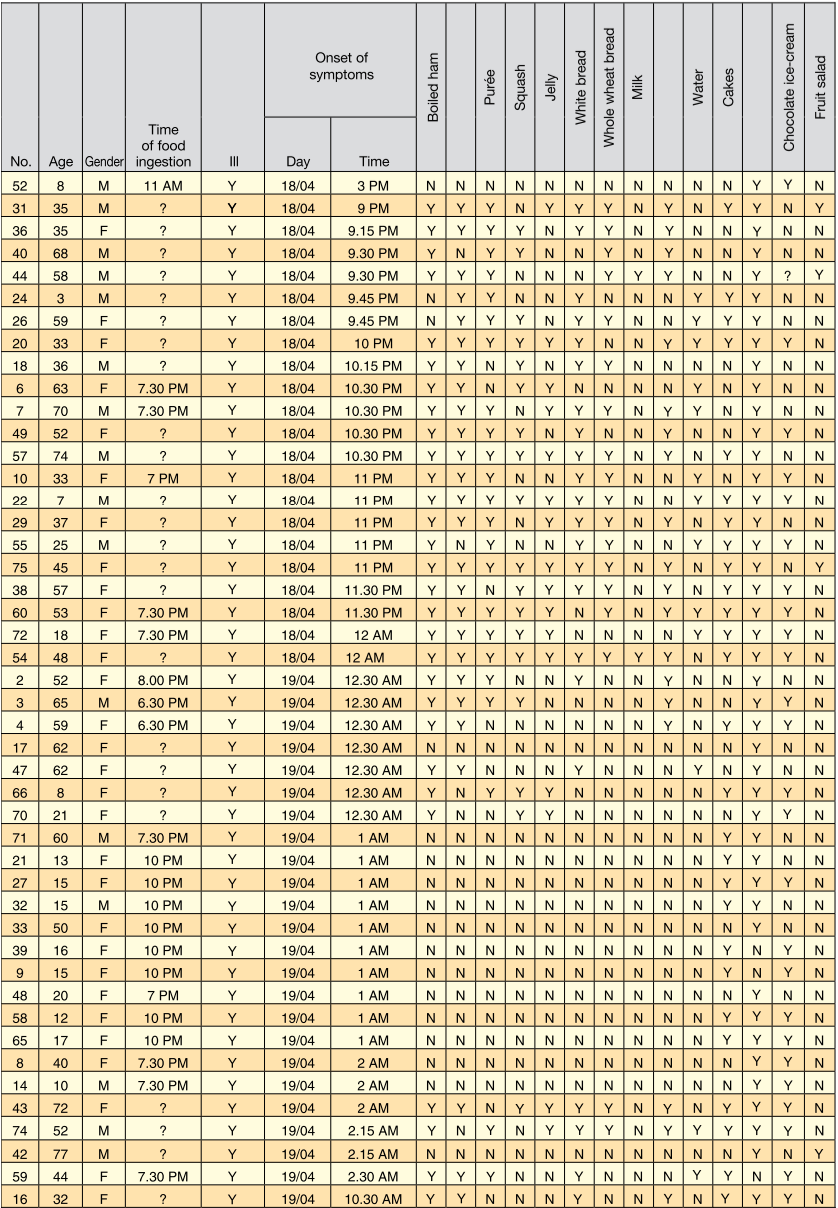
Dinner had been prepared simultaneously by several people and had been served in the club yard between 6 p.m. and 11 p.m. The meals had been placed on tables and eaten during a period of several hours. All 75 interviewed persons were asked about the time of onset of symptoms, and the meals and beverages they had. A table was created using these data (see the Appendix in Chapter 10). The exact time of food ingestion could be established in only about half of the cases.
3.1. Use of Rates: Vital Signs of a Community
Rates in Preventive Medicine
Rates are a fraction representing numbers of cases of specific conditions over the number of people in a specific population group, multiplied by an even number depicting the population at risk (Box 2). Rates facilitate the comparison between the reality of one community and that of others. They also help assess through time the success of interventions in a given population.
BOX 2: The “patient” of preventive medicine
- Groups, not individual patients
- “Vital signs” = Rates of disease
- Rates = persons x even number persons at risk
- Even number: represents the size of the population (1,000, 10,000 or 100,000)
Determining rates is a skill that many clinicians do not use on a daily basis, but it is critical to understanding health problems in a community. Without this data, scarce resources will not be used rationally for the good of the community. This is particularly critical in post-disaster scenarios where resources, such as time, are more constrained than usual.
To obtain rates, one must have both a numerator and a denominator. The numerator is the number of cases of a specific type of problem, and the denominator is the number of people in the community who are at risk for the problem. The resulting number can be reported as a fraction, a percent, or a rate. All of these convey useful information and can be converted from one to another. Using a rate is the way that most public health practitioners “speak” to each other and is probably the most useful (Box 3 and 4).
BOX 3: Rates
Example: Children younger than 5 years of age with diarrhea
Town A: 304 cases of diarrhea
Town B: 1054 cases of diarrhea
Which town has more problems with diarrhea?
BOX 4: Rates: a numerator and a denominator
Town A: 1597 children <5 years of age
Rate: \( 304/1597 * 10000 \) = 1904
Town B: 12,818 children <5 years of age
Rate: \( 1054/12,818 * 10000 \) = 822
Rates of diarrhea per 10,000 children younger than 5 years.
The value of a rate is dependent on the quality of the data that go into its creation. For accurate numerators, cases must be defined clearly so that a busy clinician can easily categorize problems. For example, a typical case definition would be 3 or more watery stools for a diarrhea case. Consistency in defining cases is key to ensuring the comparability of rates from different areas or following them over time.
Equally important to determining accurate numerators are accurate and descriptive denominators. For this, basic demographic information is needed, such as the total number of people affected in the community and the population structure, including gender breakdown and number of people in specific age groups.
In a disaster scenario, the simplest way of subdividing groups by age is to classify them under 5 years, 5-15 years and over 15 years. It might be useful to subdivide this last group into 15 to 60 and over 60.
Crude Mortality Rate
The most critical rates to follow after a disaster are mortality (death) rates. The daily crude mortality rate (CMR) is determined by taking the total number of deaths in a population (community), dividing it by the total number of people in that population, and multiplying that number by 10,000 (Box 5).
BOX 5. Crude mortality rate (CMR)
(Total number of deaths in a group ÷ Total number of persons in this group) × 10,000
Expressed as deaths per 10,000 persons per day. The objective is <1/10,000/day
For example, if a community has a population of 15,955 and it experiences 49 deaths in 7 days, the CMR will be 49 / 15,955 x 10,000 = 30.7 deaths per 10,000 people in one week. To arrive at the daily CMR, which is the international standard for gauging disaster severity and effectiveness of response, divide this number by 7 to get a daily CMR of 4.4 deaths per 10,000 people per day.
Attack rates are incidence rates; i.e., they reflect the number of new cases in a given population.
The mortality rate of children under 5 years, i.e. the number of deaths in children younger than 5 years, is another important measure to assess the severity of a disaster and the capacity for response. It is important not only because it shows the effects of the disaster on children, but also because children are the most vulnerable members of society. This age group is usually called the “sentinel population,” because changes will become evident sooner than in other age segments. Health-care workers should worry when the mortality rate reaches 2 deaths/10,000 children age <5/day.The situation is considered severe when this rate mounts to 4 deaths/10,000 children age <5/day.
Attack rates are also usually utilized during disaster situations. These rates express the relation between the number of newly diseased persons (cases) and the total population at risk. Attack rates are incidence rates, i.e., they reflect the number of new cases in a given population. On the other hand, prevalence rates measure the proportion of cases of different diseases in a given population. They express the specific weight of a given disease with relation to the aggregate of all diseases, and allow establishing priorities in the management of diseases and the use of human resources. However, in contrast to incidence rates, prevalence rates do not reflect the risk of an epidemic.
4. Evaluation of the Needs During an Emergency
Population Health Evaluations Including Emergency Needs Assessments
OBJECTIVES
- Recall major components of a population evaluation: demographics, predisaster health conditions, an emergency needs assessment, health-care system evaluation, and establishing a surveillance program.
- Complete the major components of an emergency needs assessment. Draft disaster response plans using community resources (transportation, communication, security).
Population Evaluation
Pediatricians can facilitate post-disaster recovery in their communities by helping to assess local population conditions. It is important to obtain as much hard data as possible – do not depend on speculation. Too often, disaster relief efforts are hindered and resources squandered by well intentioned people acting without the background of sound epidemiological data. Box 6 describes the components of a population evaluation.
BOX 6. Population evaluation
- Demographic data
- Measures of health status prior to the disaster
- Evaluation of the emergency needs
- Establishment of a morbidity/mortality surveillance system
Demographic Data
In a disaster, collecting data on population characteristics (number, age groups, ethnicity, gender) is critical. The crudest form of counting people is by air. This is by far the least accurate way of assessing the scope of a disaster, but it may be all that is possible in some situations. Visual estimates from the ground may be used as well to get a quick count of the affected population.
More accurate method to assess the affected population and its structure is by using standard sampling techniques, such as systematic household sampling. The most accurate way to gather demographic information is to count all individuals and list them by age group and sex. Vulnerable groups (such as children under 5 years and/or without a family, breastfeeding mothers, pregnant women, the elderly, and the injured) need particular attention and must be identified.
Without accurate demographic data, it will be difficult to determine the true nature of what is happening in a community and scarce resources may be wasted.
Although counting people and rate demographic data, it will be difficult to determine the true nature of what is happening in a community, and scarce resources may be wasted.
Pre-disaster Health Conditions groups may be tedious, this is a top priority (Box 7). Humanitarian agencies such as UNHCR, WFP, OCHA register beneficiaries so consider obtaining population denominators from such agencies.
BOX 7. Demographic data
- Affected population count (high priority)
- Visual estimation
- Sampling
- Census
- Population structure: male/female and age segments (<5 years, 5-15 years, >15 years)
- Risk groups: young children, pregnant and lactating women, elderly and wounded people
Read the case and consider your answers. Additional case questions appear in later chapters; answers are provided in Chapter 8, Case Resolution.
Case (Cont.):
- How does the information on the incubation period (in addition to the clinical data) contribute to the differential diagnosis of the disease?
- Identify the vehicle or vehicles of the infection.
4.1. Pre-disaster Health Conditions
Baseline Health Data and Preparedness
Baseline health data may be obtained from local health authorities. Immunization records provide a good source of demographic data. Health workers can provide basic information on what type of health problems were present in the pre-disaster community as well as the areas that are most likely to be affected, such as the most vulnerable households.
Pediatricians can maximize their disaster preparedness by being active in preparing community health plans and taking the lead in helping with community disaster drills. The ideal situation would be for all public and private health care workers to meet periodically to discuss community health problems and practice disaster drills. This would increase their knowledge of the community and its health problems, and would allow for relationships to be built between the public and private sector before a disaster strikes.
4.2. Emergency Needs Assessment
Emergency Needs Assessment
A needs assessment looks at what a community lacks as well as what resources and capacities it can use to address problems. The objective of a needs assessment is to identify gaps between current community needs and resources.
Whenever possible, it is preferable to close the gaps between needs and resources by mobilizing local resources immediately instead of waiting for outside assistance.
Emergency needs assessments (also called rapid needs assessments) are focused on those needs that can ameliorate the greatest amount of morbidity in the community (Box 8).
BOX 8: Critical items in the evaluation of the emergency needs
- Drinking water
- Nutritional status
- Shelter
- Basic sanitation
- Local environmental conditions
- Public health needs
Security, transportation, and communication are also key elements of an emergency community needs assessment; however, these components may fall outside the traditional healthcare realm. They will be covered in greater detail under “Conditions of other community resources” at the end of this section.
Water
Water is critical to survival and must always be a top priority. The quantity of water is a higher priority than quality in the immediate post-disaster scenario. Providing clean water will do more to prevent the spread of disease than any other preventive medicine intervention. An estimates of water quantity needs only for drinking varies from 3 to 4 liters/person/day. However, the water needs will increase to 15 to 20 liters/person/day when cooking, cleaning, laundry, and personal hygiene are taken into account. The immediate identification of water sources, ways to protect these resources and methods to improve water quality are top priorities. Water purification systems may eventually be provided by relief agencies. If there are immediate concerns about the safety of the water, then it can be chlorinated by adding 2 drops of bleach (sodium hypochlorite solution) per liter of water.
Nutritional status
Nutritional assessments take into account community needs as well as local resources. Again data, not speculation, is needed. The recommendation for caloric needs in a displaced population is 2,100 Kcal/person per day. Other elements of the nutritional needs assessment include food availability, nutrition quality including availability of adequate micro-nutrients, food security, distribution throughout the community, and cultural factors that affect nutrition.
Providing clean water will do more to prevent disease spread than any other preventive medicine intervention.
Common sampling techniques for surveying children’s nutritional status (or other health condition) include random selection (simple or systematic) or cluster sampling. Simple random selection can be done if all the children can be identified, such as by immunization records or a camp census. They are assigned a number and then a random number table is used to select those who will be evaluated for nutritional status.
Systematic random sampling is done by checking every nth household to get enough children for a representative sample. This is useful if the households are reasonably neatly ordered, such as ordered in rows of tents. The interval between each household that is sampled (n) is determined by the total number of households in the community divided by the number of households you wish to sample. For example, to check the nutritional status of children in 450 households out of a total of 2,800 households, you would check every sixth household (2,800 divided by 450). The first household to be sampled would be determined by randomly selecting a number between 1 and 6. Survey teams would then check the nutritional status of children in every sixth household, beginning with the randomly selected one.
Cluster sampling is a statistical sampling technique that is used for large numbers of people and is beyond the scope of this discussion. A public health professional with training in epidemiology or a standard text on this subject could be used to design a survey using cluster technique.
If random selection (simple or systematic) is used, a sample size of about 450 children is needed. If cluster sampling is used, the sample size should be of about 900 children for an accurate population estimate. If the community size is small enough, it is more accurate to simply check all the children who are in the sentinel population age range.
It is important to bear in mind that the sample size will depend not only on the population size but also on the frequency of the phenomenon being investigated; i.e., the prevalence of this phenomenon in the community.
Shelter
For shelter, the WHO recommends 3.5 to 4 squared meters (m2) per person as the absolute minimal amount of floor space for a displaced population. A rapid assessment of available remaining space will identify any disparity between needs and capacity. Predisaster planning should emphasize the use of community spaces such as schools, churches, and assembly halls for emergency shelter.
Basic sanitation
Basic sanitation is aimed at preventing spread of communicable diseases from indiscriminant defecation. Feces are a concentrated source of human pathogens and can lead to explosive outbreaks of diarrheal diseases. In a post-disaster scenario, effective control of human waste is a top priority. One person can contaminate water used by thousands, and flies can spread fecal material to food supplies, rapidly creating hundreds or thousands of cases of food and waterborne illness.
Local environmental conditions
Conditions that affect community health, such as smoke, chemical spills, floods, landslides, collapsed buildings, terrain slopes, drainages, and insect vectors, are all important to assess during disaster situations.
Organized plans for signaling an emergency and identifying a specific location to convene as a group would lead to rapid mobilization of all health-care workers in case of an emergency.
Health needs
The emergency assessment of health needs is focused on mortality rates and the chief causes of morbidity. Death is the most severe negative health outcome and it must be tracked carefully to understand what is happening in a community. To provide the most accurate information, mortality data should be reported by age, sex, and cause of death.
Morbidity data is also of key importance for understanding community health needs.
This data is captured by using patient logbooks or records that record age, sex and chief diagnosis of the patient. This data can be rapidly analyzed to gain an understanding of the chief health threats to the community and used to plan the use of resources accordingly.
4.3. Healthcare System Evaluation
Evaluation of Health-Care Resources
While not a part of the traditional emergency needs assessment, an evaluation of community health-care resources, including human resources, medical supplies, equipment, surgical capability, emergency department and primary care capacity and the condition of health-care buildings, is also an important part of the process following a disaster. From the preventive medicine standpoint, evaluation of the availability of vaccines and the condition of the cold chain is extremely important.
Evaluation of the health-care system requires pre-disaster knowledge of community resources. By joining with public health officials and disaster planning committees, pediatricians and other local physicians can be included in community health-care worker rosters and will learn where emergency medical supplies are stored. Organized plans for signaling an emergency and identifying a specific location to convene as a group would lead to rapid mobilization of all health-care workers in case of an emergency. Identifying additional areas for handling surge capacity and the staffing of these additional treatment areas is important. For example, with a pandemic influenza outbreak, current healthcare facilities can become overwhelmed. Identifying alternate care facilities in each community and regionally may be needed to meet demands. Predisaster planning by delegating responsibilities for assessing the condition of local hospitals and clinics and determining available medical supplies will avoid confusion and wasted efforts.
4.4. Establishing a System of Morbidity and Mortality Surveillance
Disease Recording and Reporting
After a disaster, it is critical that all health-care workers, both private and public, join together to form an integrated and coordinated system that records and reports diseases. This is one of the most important roles of health workers who are engaged in a traditional clinical consulting mode. To the clinician who is working long hours trying to treat as many patients as possible, gathering data may seem like a waste of time, but it is crucial for planning disaster response.
The ideal situation would be to have every health worker record the age, sex, and diagnosis of each patient. This information should be collected and recorded in a systematic way and provided in a timely manner to public health authorities so they can analyze it and rapidly respond to emerging health threats. In a sophisticated health-care system, electronic medical records can greatly facilitate this data acquisition.
4.5. Conditions of Other Community Resources
Transportation and Communication Resources
Transportation and communication are critical components of the disaster response strategy. Two-way communication systems such as radios, telephone, and Internet capability are critical for disseminating information, communicating among disaster workers, and planning outside help. Use mass media for providing emergency instructions and health education. The condition of roads, waterways, and landing strips/fields is also important for evacuating people who are injured and receiving emergency aid. Motor vehicles, fuel sources, and boats may be important for rapidly establishing a logistical bridge into disaster-affected areas.
Security
Security is another need that is sometimes overlooked by health workers. Security may be needed to carry out the initial rapid emergency needs assessment or to maintain control of victims seeking basic supplies or health care access. While health workers probably will not be called upon to establish security for disaster affected populations, they can facilitate protection from crime, looting, and exploitation by sharing information regarding criminal activity with security forces. Health workers can also provide security for unaccompanied minors by quickly taking control of these children and keeping them safe from exploitation until family reunification or another permanent solution can be achieved.
Epidemic preparedness and outbreak response
Given the Ebola epidemic in West Africa, Hepatitis E outbreak in South Sudan, Yellow Fever in Sudan and the repeated cholera and malaria outbreaks in various disaster situations and influenza epidemics it is important to evaluate whether a clinical facility has an adequate epidemic preparedness plan. Is there a current plan for your facility? How does this plan integrate with regional plans? Have you considered contingency plans for yourself or your coworkers in terms of providing child care or family member care if they become sick? Additional staffing needs may be large. Is there a requirement for all your facilities health-care workers to be vaccinated, and do those plans have a method in place for those who refuse vaccination to prevent the spread of disease (nonclinical work, rules for wearing proper masks)? Depending on the epidemic characteristics, certain populations may be more affected than others, or there may be vast numbers of mildly infected patients with few critical patients or an outbreak with many critical patients. Establishing triage systems to sort these patients, a daily surveillance of the types of these patients and degree of illness, as well as antibiotics, anti-malarials, intravenous fluids, safe blood masks, vaccines, anti-virals should be addressed. Finally, establishing “alternate care guidelines” can provide a framework for dealing with a potentially large number or patients in a system that may become quickly overwhelmed. Resource allocation, ethical considerations and the legal channels to enact these “alternate care guidelines” should ideally be spelled out a priori.
5. Post-Disaster Intervention Priorities
OBJECTIVES
- Establish emergency intervention priorities following a disaster.
- Describe how the modes of disease transmission affect the intervention priorities after a disaster.
Modes of Disease Transmission
Post-disaster living conditions frequently enhance the transmission of infectious diseases. Understanding how these conditions pose health threats will help set priorities for public health interventions. The most common modes of transmission after a disaster are fecal-oral, respiratory, and vector borne. Fecal-oral transmission can occur by having human waste enter into the water supply by indiscriminant defecation or by flooding, by flies carrying feces on their feet to food sources, or from unwashed hands.
Fecal oral transmission has the greatest potential for rapid spread of infection through a displaced population, particularly if the water supply becomes contaminated.
The respiratory route is enhanced by the crowded conditions that frequently follow a disaster. Also, respiratory irritants such as smoke from open cooking fires may increase predisposition towards the spread of respiratory pathogens. Vector-borne illnesses such as malaria and dengue frequently increase following disasters, particularly floods or hurricanes because standing water increases mosquito breeding.
Infections are usually referred to when the notion of transmission is being discussed, because infection transmission is easier to prove objectively. In contrast, the epidemiologic evidence of causality in the transmission of noninfectious diseases is more difficult to demonstrate. An example is lung cancer associated with cigarette smoking.
There are four modes of transmission of infectious diseases: contact, common source, airway transmission, and transmission by vectors.
Contact
This necessitates a connection between the host and the infectious agent that causes the disease. The contact can be direct, indirect or through droplets. Direct contact involves person-to-person contact, as in the case of the fecal-oral route, in which the microorganism contained in the feces of an infected person is transmitted, due to defective hygiene conditions, to another person, usually another household member. Examples: hepatitis A, Salmonella, Shigella. An additional example is the contact with a Staphylococcus aureus infected wound. Indirect contact is through an inanimate object. Example: hepatitis B, due to the shared utilization by family members of objects such as tooth brushes. Finally, the contact through droplets is the person-to-person transmission through droplets emitted by the mouth or nostrils. The longest distance that droplets travel in the air is approximately 3 yards. Examples: measles, chickenpox, streptococcal disease.
Common Source
A microorganism or a toxin can cause disease in one or several persons from a common source that contains the infective agent. Example: gastroenteritis outbreaks resulting from contaminated food (ice cream, mushroom sauce) (Box 9).
BOX 9. The most common sources for disease transmission
- Water
- Food
- Mosquitos and flies
- Blood products
- Intravenous administration practices
Transmission through the Air
Microorganisms can travel more than 3 yards in the air from the source of infection. Traveling microparticles usually result from the evaporation of drops emitted by the source of the disease. Examples: tuberculosis (through the cough of a diseased person), psittacosis (from a diseased fowl to a person), Q fever (from contaminated products; can travel several miles), and Legionella (through air-conditioning systems).
Transmission by Vectors
Transmission by vectors can be external or internal. In the external transmission, the vector carries the unmodified infective agent on its body. Example: flies carry Salmonella acquired from contaminated feces and deposit the bacteria on food that is later ingested by the host (human being or animal). In the internal transmission, the microorganism travels inside the body of the vector, where it may remain unaltered (Yersinia pestis is ingested and then eliminated unchanged) or may be modified, as in Plasmodium falciparum transmission by the mosquito.
Recognize that transmission can occur by one or several modes (Table 1).
Select to expand to see each transmission type. For printing, expand all sections before printing.
TABLE 1. Most frequent diseases during disaster and their forms of transmission
Fecal-oral
| Bacteria | Salmonella Shigella Escherichia coli Vibrio Cholera |
|---|---|
| Viruses | Hepatitis A and E Rotavirus |
| Other | Pinworms Giardia lamblia Ascariasis |
Airway
| Bacteria | N. meningitides S. pyogenes S. pneumoniae |
|---|---|
| Viruses | Respiratory syncytial virus Varicella zoster Measles Influenza |
| Other |
Skin
| Bacteria | S. pyogenes S. aureus |
|---|---|
| Viruses | Varicella zoster Herpes simplex |
| Other | Lice Scabies Ringworm Hookworm |
Blood, urine, saliva and other body fluids
| Bacteria | Syphillis (T.Pallidum) Gonococci (N. Gonorrhea) Chancroid (H.Ducreyi) |
|---|---|
| Viruses | Hepatitis B and C Human immunodeficiency (HIV) Cytomegalovirus |
| Other | Chlamydia trachomatis |
Mosquitos and other vectors
| Bacteria | |
|---|---|
| Viruses | Malaria, Leishmania |
| Other | Yellow fever, Ebola, other hemorrhagic fevers |
Read the case and consider your answers. All answers are provided in Chapter 8, Case Resolution.
CASE (cont.)
- Determine the future investigations that should be carried out.
- What control measures would you implement?
5.1. Public Health Priorities
Post-Disaster Health Interventions
The objective of post-disaster health interventions is to minimize death and prevent excess disease. Another public health priority is to facilitate community preparation for future disasters. Ideally, all interventions are guided by a thorough emergency needs assessment and ongoing evaluation of the team’s effectiveness during a disaster situation.
Among the survivors of the immediate inciting event, the leading causes of morbidity in disasters typically are diarrhea and acute respiratory infections.
Immediate public health interventions include the following priorities:
- Provide safe drinking water
- Control human waste
- Protect food supply
- Vector control
- Provide adequate shelter
Provide Safe Drinking Water
Providing sufficient quantities of clean drinking water is usually the highest priority of all disaster relief efforts. Effective water purification programs will likely have a greater impact on community death and disease rates than any other single intervention. To be effective, drinking water programs must be accepted by the community, so factors such as taste and convenient access to the purified water source must be taken into account. For long-term planning, water purification programs must be sustainable by the community once the disaster is under control.
Simple field treatment of water may improve quality and decrease waterborne infections. Covering and allowing sediments to settle will improve the quality and decrease amount of chlorination needed to purify water. Sand filtration by allowing water to percolate through stones and sand contained in a 55 gallon barrel will also improve quality of water. Bulk chlorination, when available, is another way to provide clean water to large numbers of people. Reverse osmosis units, such as those used by military, can provide thousands of gallons of pure water but are expensive, require expertise to operate, and take many days to deliver to a community, costing valuable time.
Boiling takes time and effort. Cleaning water by adding bleach or chlorine at the household level relies upon motivation, efficient distribution of cleansing products, and most important, a fair amount of education to do it correctly.
The least effective means of cleaning water for consumption is relying on the individual users to do it themselves by boiling or adding chlorine to the water.
Utilizing an effective distribution system is equally important as having clean water. No matter the quality of water at the source, it must arrive to the end users in some fashion. Clean, covered storage tanks are a top priority as well as a means to transport the water to community members.
Control Human Waste
It is best to use a family-centered approach to establishing portable lavatories.
Take into account the special needs of children when planning for community sanitation programs. Children are more likely to defecate indiscriminately and may not use a portable lavatory that is inconveniently located, frightening, or does not meet their physical needs. Soap and water for personal hygiene are a lower priority when compared with drinking water supply and the elimination of feces. However, after drinking water requirements have been covered, it will be important to provide soap and water for personal hygiene to prevent the spread of infectious diseases. A minimum of 7 liters of water per person daily is needed for covering hygiene requirements.
Protect Food Supply
Developing a plan for protecting the food supply should occur in disaster preparedness. Securing community resources and safely storing and protecting emergency rations are important details to work out in advance and should include all key agencies involved with disaster planning. Protecting food preparation from contamination is a high priority. Basic measures for preventing food-borne illness include:
- Using drinking water for food preparation
- Strict hand washing by food handlers
- Keeping food preparation areas and utensils as clean as possible
- Control of flies and other vectors
- Proper cooking, storage and serving techniques.
Additionally, providing health education information may be necessary to help community members prepare and use food resources safely.
Provide Adequate Shelter
WHO recommends at least 4 square meters of floor space for each person in an emergency shelter. Shelters are more effective if they keep families and other traditional community groups together and are close to resources such as food, water, lavatories, medical care, and transportation. When homes are destroyed, it is far better to locate shelters as close to or within the pre-existing community whenever possible.
5.2. Surveillance Cycle
The Use of the Surveillance Cycle to Guide Use of Resources
OBJECTIVES
- Use the surveillance cycle to help make rational health-care decisions.
- Understand the key role that primary care doctors and pediatricians play in the compilation of quality information, while simultaneously attending individual patients.
- Use this information in an appropriate way for decision making.
Surveillance Cycle: A Powerful Public Health Tool
After the emergency assessment is completed and disaster recovery operations have started, ongoing surveillance will evaluate emerging population needs. Surveillance is defined by the U.S. Centers for Disease Control and Prevention (CDC) as “...the ongoing, systematic collection, analysis and interpretation of public health data essential to the planning, implementation and evaluation of public health practice, closely integrated with the timely dissemination of these data to those who need to know. The final link is the application of these data to prevention and control. A surveillance system includes a functional capacity for data collection, analysis and dissemination linked to public health programs.”
The surveillance cycle essentially consists of gathering data that are critical for monitoring ongoing health needs, analyzing and interpreting that data in a timely fashion, providing feedback to those who need to know, and taking actions based on these data (Box 10). After an action is taken, the cycle is repeated to re-evaluate the effectiveness of this action (Figure 1).
Box 10. Important Data
- Deaths
- Severe morbidity or diseases that are frequent in the community
- Rapid detection of selected conditions or infections, such as cholera cases, malnutrition, malaria, and severe trauma
- Document spread of infections by collecting list of affected person
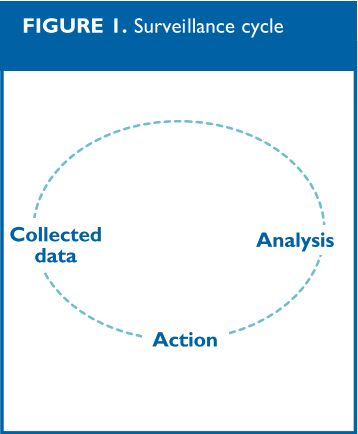
Figure 1
The most important point of the surveillance cycle is making sure that data are used. Unused public health data that sit gathering dust is a waste of resources. For this reason, there needs to be a clear link between data gathered by clinicians doing face-to-face consultation and policy implementation based on that data. If busy clinicians feel that keeping a patient logbook only adds more work to their day and has no impact on patient health, they will quickly stop gathering the data. This is where a breakdown between clinical and public health services frequently prevents optimal use of the surveillance cycle.
5.3. Preventive medicine roles of pediatricians following a disaster in their community
Pediatricians’ Role in Preventive Medicine
Pediatricians, whether in public or private service, can assist disaster recovery in their communities in many ways. These need not be limited to simply seeing children in consultation; with adequate preparation, pediatricians and other physicians and nurses can fill many important roles, from assisting with search and rescue efforts to conducting population surveys. Their effectiveness will largely depend on personal preparation and their integration into community pre-disaster planning strategies (Box 11).
Box 11: The pediatricians’ role in preventive medicine
- Before a disaster: not limiting themselves to direct patient care
- Evaluations after the disaster:
- Nutritional evaluation
- Children’s requirements
- Collaboration in disease surveillance:
- Design of surveillance systems keeping children in mind
- Collaboration in the collection and analysis of data
Children form a large proportion of the population and because children are one of the most vulnerable groups during a disaster, it makes sense to have pediatricians serve as leaders in disaster response and preparedness programs. Drills should involve children as mock victims, and should represent the ages and numbers representative of the population at large. Advance planning for meeting children’s special nutritional, psychological, and developmental needs will likely happen only if pediatricians are involved in every aspect of disaster planning. By teaching other health workers, such as nurses, general practice doctors, and lay community health workers, pediatricians can disseminate their knowledge of children’s special needs throughout the disaster response community.
Drills should involve children as mock victims, and represent the ages and numbers that are representative of the population at large.
Pediatricians in private practice may need to go out of their way to meet with public health, military, and other governmental officials to offer their services in pre-disaster planning. Waiting to act “ad hoc” after a disaster strikes is a recipe for wasted effort and represents an inability to make a meaningful impact on community recovery.
Pediatricians and the Surveillance Cycle
Even if pediatricians work primarily in their traditional capacity of clinical consultation, they may still have a significant role to play in preventive medicine by making sure that a functioning surveillance cycle is in place. Crucial points of the cycle would include establishing an adequate patient logbook or record that captures important disease data and stratifies data to specific age and sex groups. This is where the surveillance cycle begins, with clinicians seeing individual patients. If they do not capture this data, public health decisions will be based on speculation, not facts.
Next, pediatricians can ensure that individual patient data are shared with public health authorities in a timely fashion, which will allow analysis and quick response to rapidly emerging public health needs. Pediatricians who handle their own preliminary data analysis by reviewing patient logbooks on a daily basis and looking at disease incidence data in terms of rates will allow quicker and more effective interventions and recommendations for resource allocation. Finally, by developing and maintaining effective communication with public health leaders, pediatricians can ensure that wise decisions are made regarding the care of children in their communities.
6. Summary
Conclusion
Pediatricians have much to offer their communities in disaster preparedness and response. Knowledge of children’s medical needs and a natural tendency to be advocates for children are pediatricians’ greatest assets. After a disaster, basic preventive medicine and public health is generally a higher priority than providing clinical consultation for individual patients, and this will help increase pediatricians’ ability to effectively respond to a disaster in their community.
Good preventive medicine techniques involve thorough population evaluation and needs assessments, and using these data to guide initial disaster response. Setting up a functional surveillance system will help evaluate the adequacy of disaster response interventions and will alert clinicians and public health officials to emerging threats to community health. Gathering and using data to intervene at the community level will help ensure the best possible outcomes for entire communities when a disaster strikes.
7. Suggested Readings
References
- Brown V, Moren A, Paquet C. Rapid Health Assessment of Refugee or Displaced Populations 2nd ed. Epicentere Médecins Sans Frontières, Paris, 1999.
- Carrasco, P. Vaccines in Disaster Situations: Recommendations of the PAHO/WHO Special Program for Vaccines and Immunizations. These recommendations can be found at the following Web site:
www.paho.org/English/DD/PED/te_vacc.htm (as of 15 June 2005). - Chin J. Control of Communicable Diseases Manual, 17th ed. American Public Health Association, Washington DC, 2000.
- Hansen R K. Preventive Medicine in Humanitarian Emergencies. In: Military Medical Humanitarian Assistance Course Manual, pp.VI 2-20, Uniformed Services University of Health Sciences, Bethesda MD, 1998.
- Mandalakas A, Torjesen K, Olness K, ed. Helping the Children: A Practical Handbook for Complex Humanitarian Emergencies. Johnson and Johnson Pediatric Institute and Health Frontiers, Kenyon, MN, 1999.
- Noji E. ABC of Conflict and Disaster: Public Health in the Aftermath of Disasters. British Medical Journal; 330:1379-1381.
- Pan American Health Organization. Vigilancia Epidemiológica Sanitaria en Situaciones de Desastre: Guia para el nivel local. Washington DC OPS/PAHO 2002.
- Redmond A. ABC of Conflict and Disaster: Needs Assessments of Humanitarian Crises. British Medical Journal, 2005:1320-1322.
- United States Agency for International Development Office of Foreign Disaster Assistance. Field Operations Guide, ed.3.0. Washington DC, 1998.
- World Health Organization. Handbook for Emergency Field Operations, Geneva, 1999.
8. Case Resolution
Case Resolution
Case 1
The situation described in the case presentation can be considered an epidemic, taking into account the number of cases observed in the club, which would not to be expected. It is important to remember that an epidemic is defined as an increase in the number of cases at a given time and in a given place, as compared with those observed at the same time and place in previous years.
Case 2
Diseases that can be considered in the differential diagnosis of an outbreak of acute gastroenteritis include:
- Bacterial: Salmonella typhi, Shigella, Staphylococcus aureus (toxin)
- Viral: Rotavirus
Case 3
Incubation times associated with the different potential etiologic agents vary. Therefore, the estimation of the time interval between food ingestion and the onset of symptoms may help identify the probable etiology of this epidemic outbreak.
Case 4
The likely vehicle is one of the foods ingested during dinner.
Case 5
It would be appropriate to culture fecal samples from the individuals responsible for the preparation and distribution of meals, as well as from the sites in which meals were prepared and stored. It would also be adequate to obtain samples for culture from meals served during dinner, if they have been stored or not yet eliminated.
Case 6
Implement strict hygiene measures in the club kitchen, and insist on careful hand washing by the persons responsible for the preparation of meals. If a carrier of one of the potential etiologic agents of the described outbreak is identified, isolate the carrier until the pathogen is eradicated.
9. Book Review
Review Questions
Chapters 1 - 3: Overview, Introduction, and Gathering and Using Population Data
- How can preventive medicine be characterized?
- How is a rate defined? What purposes can rates serve?
- What is an epidemic?
- What factors should be taken into account for the control of an outbreak?
Chapter 4: Evaluations of the Needs During an Emergency
- What are the principal factors based on which a population is evaluated?
- How are demographic data obtained?
- What is the best source of data to determine the health conditions of a population before a disaster?
- What are the key factors for assessing requirements during an emergency?
- How are healthcare resources evaluated?
Chapter 5: Post-Disaster Intervention Priorities and the Use of the Surveillance Cycle to Guide Use of Resources
- What are the primary modes of transmission of diseases?
- What are the most frequent sources of disease transmission?
- What disease conditions are frequent during a disaster?
- What are the public health priorities after a disaster?
- What are the post-disaster circumstances in which immunization is recommended?
- What components of the surveillance cycle are crucial for its effective implementation?
- What role do pediatricians play in preventive medicine?
10. Appendix
Information for the Case Resolution
Information for the case resolution:
Time of Symptom Onset and Food Ingestion
Time of symptom onset and food ingestion by the individuals who developed gastroenteritis
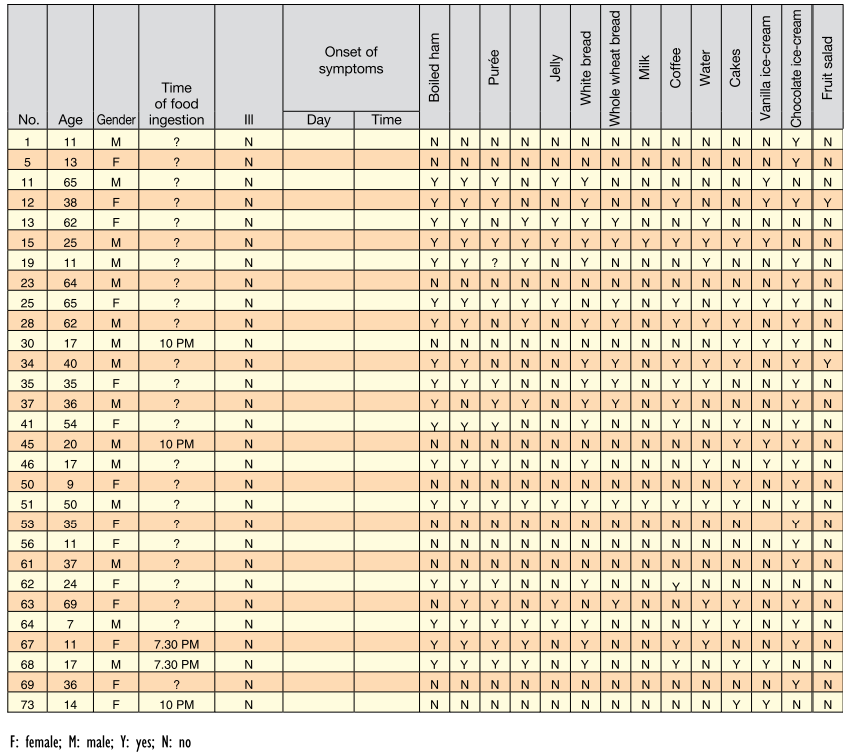
Food Eaten by Individuals Without Gastroenteritis
Food eaten by the individuals who did not develop gastroenteritis