Disasters and their Effects on the Population: Key Concepts
4. Mortality
OBJECTIVES
- Recognize crude mortality and under 5 mortality rates as a measure of disaster severity.
- Recognize the environmental factors associated with increased morbidity and mortality rates.
- Know the 5 leading causes of death in humanitarian emergencies occurring in developing countries.
Severity of a disaster
As was demonstrated in Haiti, the more fragile the pre-event health status of the affected population and the more inadequate the pre-disaster infrastructure, the more severe the disaster. Disaster severity therefore varies according to its magnitude and the vulnerability of the population.
Most diseases associated with the event can be prevented by adequate interventions, especially ensuring basic life saving needs of the population are met. This includes shelter, food, water, sanitation, health care services and security measures.
An example of this can be seen in earthquakes of similar magnitude in different parts of the world. Earthquakes in China and Haiti resulted in a large number of collapsed buildings, including schools and hospitals, related to substandard building practices in both countries, and thus a high number of casualties. By contrast, earthquakes of similar magnitude occurring in Tokyo in 2009 and Chile in 2010 resulted in far less loss of life, largely because of higher-quality construction and stricter building codes.
Crude mortality rate
When assessing the outcome of a disaster, public health officers describe its severity by the number of human lives lost using the crude mortality rate (CMR). CMR is usually defined as the number of deaths per 10,000 inhabitants per day.
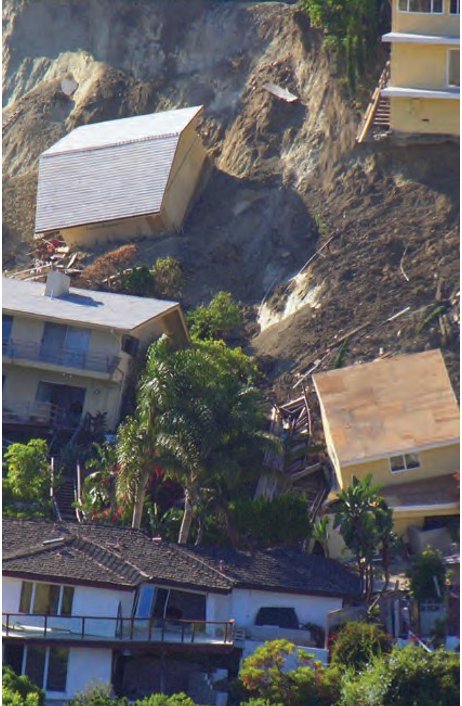
Natural disasters can result in numerous immediate deaths due to trauma
In developing countries, the reference CMR value varies from 0.4 to 0.7 deaths per 10,000 people per day. A CMR above 1 death per 10,000 people per day, or an under-5 mortality rate above 2 deaths per 10,000 children under 5 per day, is considered a humanitarian emergency.
While both conflicts and natural disasters can result in immediate deaths due to trauma or drowning, there are many preventable deaths that occur in later phases of a disaster over a longer time period.
To assess the progression of a disaster and the effectiveness of relief interventions, the CMR should be measured over several appropriate time intervals. For example, during the month following the massive movement of Rwandan refugees to eastern Zaire (present-day Democratic Republic of the Congo), the CMR in that region was 40 to 60 times above the corresponding reference value.
The CMR is usually highest during the initial phase of a disaster. Figure 6 displays the differences between baseline and peak disaster CMR experienced by displaced populations in different countries. Additional information regarding these epidemiologic measurements may be found in Module 2, “Preventive Medicine in Humanitarian Emergencies.”
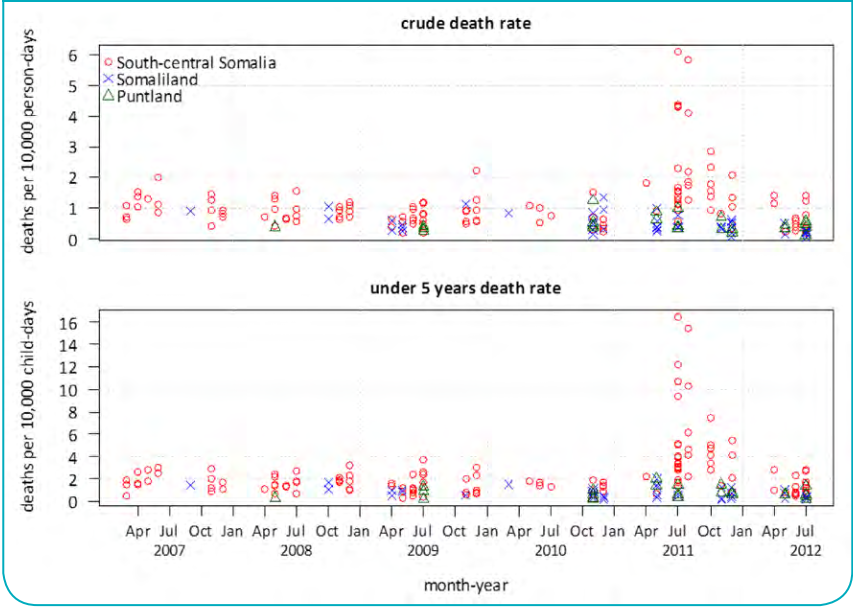
Source: “Mortality among populations of southern and central Somalia affected by severe food insecurity and famine during 2010–2012.” A study commissioned by FAO/FSNAU and FEWS NET, conducted by the London School of Hygiene and Tropical Medicine and the Johns Hopkins University Bloomberg School of Public Health.